Intraneural glomus tumor within the digital nerve: a case report
Article information

Abstract
A glomus tumor is a soft tissue tumor that arises from the glomus body, a peripheral organ responsible for regulating skin temperature. It accounts for about 1% to 5% of tumors occurring in the hand, is mainly located in the subungual region, and is less than 1 cm in size. The diagnosis is mainly based on clinical symptoms, and the main symptoms are pain at the site of the glomus tumor, pinpoint tenderness, and cold intolerance. The pain is severe and usually requires surgical resection, and the results of complete resection of the tumor are good. This case report presents a 37-year-old female patient who developed pain in the radial side around the proximal interphalangeal joint of the right second finger without any traumatic history. On physical examination and imaging, a glomus tumor of the digital nerve was diagnosed and resected. After surgery, the symptoms improved and there was no recurrence. A careful examination and accurate diagnosis and treatment are necessary for symptomatic masses.
Introduction
A glomus tumor is an excessive enlargement of the glomus body, which mainly occurs in the hands and feet where the glomus body is widely distributed. It mainly occurs in the subungual region, and cases of peripheral nerves have been reported very rarely [1,2]. The authors would like to report a case of glomus tumor that occurred within the digital nerve, in which symptoms were improved through surgery.
Case report
A 37-year-old female patient visited the outpatient clinic complaining of pain, tenderness, and sensitivity to cold and heat in the radial side region around the proximal interphalangeal joint of the right second finger, which had been felt for 3 years. There was no trauma history to the painful area in the past or occupation, and the use of the hand was considered to be routine. There was no other underlying disease such as diabetes. On examination, there was no change in the color of the symptomatic finger, the protrusion of the mass in the tender area was not clear, and the finger sensation and movement of the finger joint were normal. When palpation of the lesion site, a mass causing pinpoint tenderness of NRS (numerical rating scale) 7 was palpated subcutaneously, there was no tingling radiating along the finger. In the physical examination, it was thought that the possibility of glomus tumor was high. However, the painful area was not a site where glomus tumors commonly occur, and there was no traumatic history to suspect a neuroma and there was no Tinel sign.
To make an accurate diagnosis of the suspected lesion, magnetic resonance imaging was performed. On magnetic resonance imaging, a mass of 4 mm in diameter was identified in the radial side digital nerve around the proximal interphalangeal joint of the right second finger. In T1-weighted images using a contrast agent (gadolinium), strong enhancement was observed. The possibility of intraneural glomus tumor was considered, and mass resection was performed for diagnosis and treatment (Fig. 1).
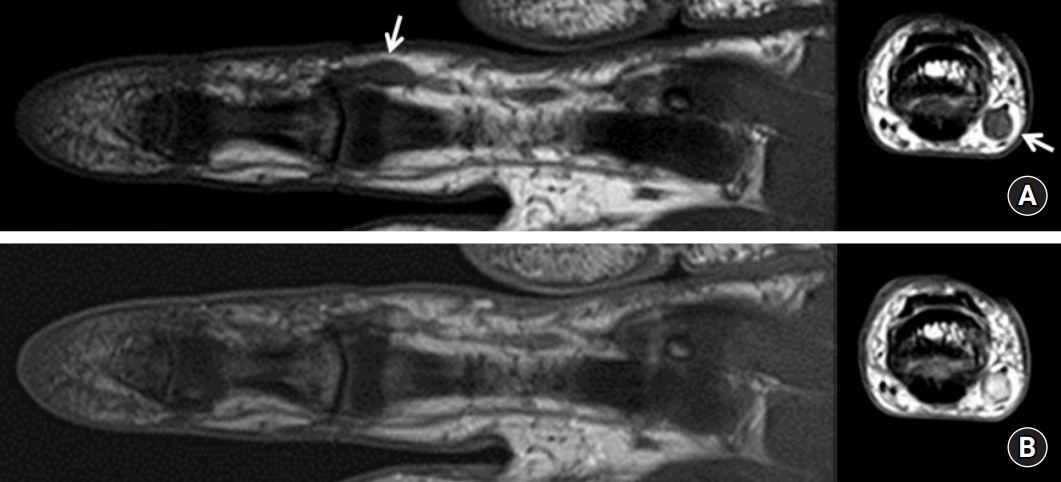
Magnetic resonance imaging of the right second finger. (A) The arrow shows a glomus tumor at the level of the around the proximal interphalangeal joint (T1-weighted coronal and axial noncontrast). (B) T1-weighted coronal and axial images using a contrast agent (gadolinium); strong enhancement was observed.
The mass was approached by making an incision in the longitudinal direction above the mass from the palmar side of finger. When approaching the mass by meticulous dissection, a relatively thick digital nerve with a non-smooth surface was observed (Fig. 2). The epineurium was dissected to expose the mass, and the mass was carefully excised while minimizing damage to the adjacent fascicle. It was confirmed as a benign glomus tumor in the pathology (Fig. 3).
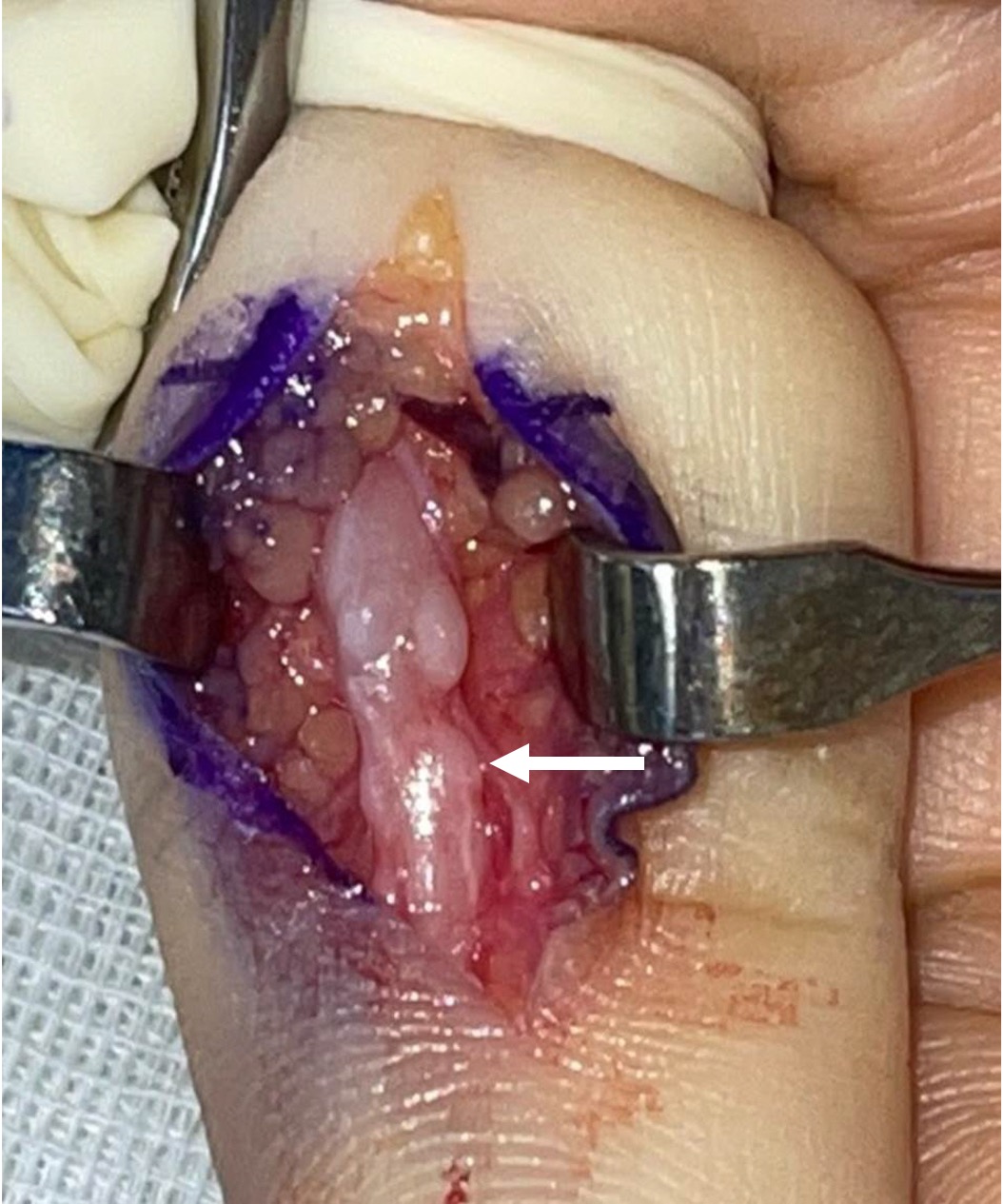
Intraoperative photograph shows the glomus tumor (arrow) within the radial digital nerve, with a relatively thick and non-smooth surface.
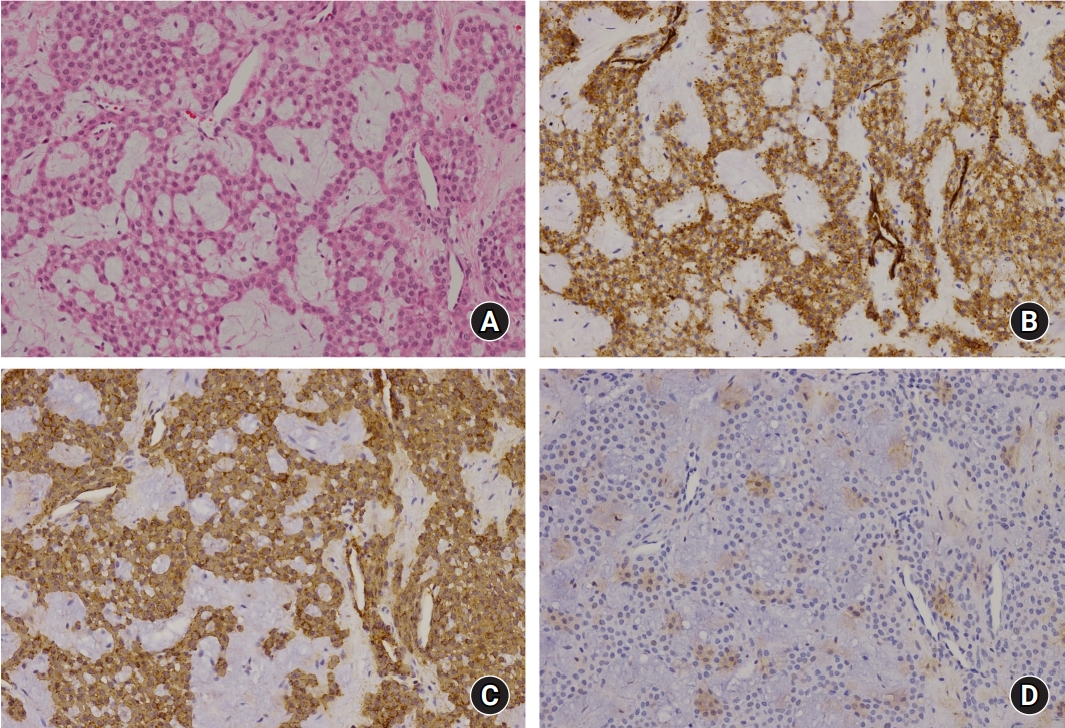
Histology findings (×200). (A) Branching capillary-sized vessels lined by endothelial cells surrounded by collars of uniform glomus cells forming nests, sheets, and trabeculae in the myxoid stroma (hematoxylin and eosin staining); positive for CD34 protein (B), positive for smooth muscle antigen (C), negative for S-100 protein (D).
Six weeks after surgery to remove the mass, the physical examination showed that the tenderness in the area where the mass was located disappeared, and there was no change in the sensation of the finger.
Discussion
Glomus tumor is an uncommon tumor originating from the glomus body. It can occur anywhere in the body where the glomus body is distributed, but the most common site is the subungal area of the finger [1,2]. In some cases, deformation or color change of the nail can be observed [3], but if the size of the tumor is small, it may be difficult to visually identify or the tumor may not be palpable. In general, glomus tumors occur frequently in the 20s and 40s and are known to occur mostly in women [4,5].
Differently, glomus tumors occurring in areas other than the fingers occur at a rate four times higher in men than in women and occur mainly in those in their 30s and 60s. In addition, there are cases where the typical symptoms of glomus tumor, such as severe tenderness or cold intolerance, are not shown, so it is often misdiagnosed in the early stage, and it takes a long time to diagnose glomus tumor [6]. The patient in this case was also not properly treated for 3 years due to an incorrect diagnosis.
Characteristic symptoms are extreme pain and tenderness when stimulated, and there are cases of complaints of severe pain in the affected area when placed in cold water due to cold intolerance [1-5]. Severe pain occurs when the mass is pressed with the head of a pin during physical examination (Love’s pin test) [1-3].
As in this case, cases in which glomus tumors develop on nerves are rarely reported, and there are cases where the typical symptoms of glomus tumors are point tenderness and cold intolerance. However, it is often accompanied by typical features of tumors arising from nerves, such as numbness, tingling sense, and radiating pain. Also, weakness or atrophy may be seen if it occurs in nerves including motor nerves [5].
Plain radiographs are usually negative, but osteolysis at the boundary between the tumor and bone may be seen. Magnetic resonance imaging using a contrast medium is used in preparation for accurate diagnosis and surgical treatment of suspected lesions due to the small size of the tumor [3,4].
In most cases, the T1-weighted image shows low signal intensity and T2-weighted image shows high signal intensity. T1-weighted images using a contrast medium (gadolinium) show high signal intensity [3]. Improvement of symptoms can be expected through complete surgical resection, but it is known that there is a possibility of recurrence [7].
Since the glomus body is not normally distributed in nerves, it is very rare that glomus tumors develop in nerves. Therefore, various hypotheses about the causes of glomus tumors occurring in nerves are classified according to the origin of the glomus body, which is the cause of glomus tumors [8]. First, it is known that a glomus tumor is caused by a normal intraneural glomus body or an ectopic glomus body, but there is no glomus body in the nerve. Second, the glomus body, which is the cause of glomus tumor, directly infiltrates into the nerve. For example, a glomus body from blood vessels directly infiltrates into nerves and can develop into a glomus tumor. Third, unspecialized perivascular cells or pericytes are generated by differentiation into glomus bodies. Cells from glomus tumors have morphological characteristics similar to those of pericytes. The pericyte is a modified smooth muscle cell distributed around small blood vessels, and the pericyte can differentiate into a tumor cell and develop into a glomus tumor [4,5,8].
For effective treatment of glomus tumor in symptomatic patients, complete resection of the tumor is required, which can relieve pain and reduce the probability of tumor recurrence. Although glomus tumors present in soft tissues are relatively easy to resection, careful microsurgical techniques are required for glomus tumors occurred within the nerves to preserve function by minimizing nerve damage during resection [7]. A glomus tumor that occurs in peripheral nerves is known as a mesenchymal tumor originating from the epineurium. In this case, when the epineurium was incised during the operation, the fascicle connected to the mass was not observed. Thus, damage to other nerve bundles could be minimized and resected completely. However, if the tumor is difficult to separate from the nerve, the connected nerve may need to be excised at the same time, and the resected nerve needs to be sutured after removal of the tumor.
Diagnosis of glomus tumors is difficult when they are small and located deep in soft tissues. If it is not common site, it may be misdiagnosed and appropriate treatment may be delayed [3]. Masses that occur in the fingers and cause pain include leiomyoma, eccrine spiradenoma, hemangioma, neuroma, osteochondroma, mucous cyst, etc [9]. In the case of tenderness and cold intolerance, glomus tumor must be included in the differential diagnosis.
Notes
The author has nothing to disclose.
Funding
None.