



Introduction
Finger striking is frequently used in children’s and adolescents’ play. Recently, the court found a teacher guilty of harassment for the ‘finger striking’ of an infant at a childcare facility. However, finger striking can cause subluxation of the sagittal band for the extensor tendon [1-3].
Spontaneous ruptures are caused by snapping, crossing a finger or crumpling paper, or light manual effort during normal daily activities. Spontaneous ruptures are located at the insertion of the sagittal band on the radial side of the extensor digitorum communis. Traumatic ruptures occur during a direct blow or powerful grasp and involve both the superficial and deep layers of the sagittal band [4].
Despite its importance in biomechanics and hand surgery, it is not known how much force finger striking may generate. The aim of this study is to elucidate the force that finger striking generates.
Methods
1. Participants
One hundred and twenty healthy Korean people without arthritis (55 males, 65 females) were volunteered.
2. Measurements
Palm area
A hand is placed on A4 paper marked with a 1-cm scale, the shape is drawn, the image is scanned, the ImageJ program is run, the image to be analyzed is loaded, and ‘Image → Type → 8-bit’ is set as the default setting. The scale is set based on a straight bar, a size of 1 cm is entered as the known distance in cm, and it is drawn according to the shape of the hand. The area fraction of the image is obtained by analyzing the size of the images on the appropriate screen by measuring the scale marked with the ImageJ program.
Circumference of fingers and wrist
The thumb at the interphalangeal (IP) joint, index finger at the proximal IP (PIP) joint, middle finger at the PIP joint, ring finger at the PIP joint, and wrist were measured.
Force generated by striking with finger flexion
Tensiometer (basic force gauge [BFG], 200 N; Mecmesin Co, Slinfold, United Kingdom). The display was measured as 0 during gauge operation, and the measurement unit was selected as newton (N). The test was carried out by measuring the displayed value of the maximum compression force identified by the symbol. The BFG digital force gauge clearly displays live load for continuous monitoring and utilizes a peak hold function to capture the maximum (Fig. 1A). In the middle finger, the average value was analyzed by measuring the force when the third finger was bent and extended with a maximum force three times with the elbow bent at 90° while sitting in a chair and the forearm and wrist in a neutral position. A 30-second break was taken between each measurement.
Force generated during extension flicking
The test was carried out by measuring the display as ‘0’ while the gauge was operating, selecting the measurement unit as N, and measuring the displayed value of the maximum compression force identified by the symbol. The BFG digital force gauge clearly displays live load for continuous monitoring and utilizes a peak hold function to capture the maximum compression reading. The force of bending and unfolding the index finger close to the load cell corresponding to the transducer part that converts the force corresponding to the hitting part into a measurable electrical output was measured three times and averaged (Fig. 1B). Similarly, the force of bending and unfolding the ring finger was measured three times and averaged. However, in the case of the middle finger, if the force generated during extension flicking (FEF) is also measured after measuring the force generated by striking with finger flexion (FFF), an error in the FEF value may occur and it may be measured as relatively less due to the added fatigue to the joint. Therefore, to prevent this bias, FEF values were measured only on the index and ring fingers.
• Index finger: The average value was analyzed by measuring the force when the second finger was bent and extended with maximum force over three times with the elbow bent at 90° while sitting in a chair and the forearm and wrist in a neutral position. A 30-second break was taken between each measurement.
• Ring finger: While sitting in a chair, the elbow was bent at 90°, the forearm and wrist were placed in a neutral position, and the force when the fourth finger was bent and extended with maximum force was measured three times. The average value was analyzed. A 30-second break was taken between each measurement.
Maximal force of exertion on grasping
The force was measured using an Electronic Hand Dynamometer (LS Networks Co. Ltd., Seoul, Korea). In fingers from the index finger to the little finger, maximum joint strengths were measured from the flexors of the four fingers, thumb, along with the forearm muscles (Fig. 2).
Statistical analysis
In this study, IBM SPSS Statistics for Windows, ver. 23.0 (IBM Corp., Armonk, NY, USA) was used. Descriptive statistics were used to investigate the general characteristics of the research subjects, and the independent sample t-test was conducted to verify whether there was a significant difference according to sex. Each measured value was expressed as a mean±standard deviation. One-way analysis of variance was conducted to verify whether there was a difference between each age group. A Scheffé post-hoc analysis was conducted for variables showing significant differences for post-hoc verification. Before checking the significance of the independent variables in a simple linear regression analysis, the goodness of fit and explanatory power of the regression model was checked. The statistical significance level was set at p<0.05.
Results
The 120 participants included 55 males (45.8%) and 65 females (54.2%). They were divided into three age groups according to their age ranges (20–29 years, 34 [28.3%], 30–39 years, 30 [25.0%], and over 40 years, 56 [46.7%]) (Table 1).
The palm area was significantly wider in males (181.4±15.1 cm2) than in females (155.1±14.0 cm2) (p<0.001). Hand surface area (HSA) was significantly wider in males (87.4±11.3 cm2) than in females (70±9 cm2) (p<0.001). The lengths of the thumb, index finger, middle finger, ring finger, and palm were significantly longer in males (5.6±0.4 cm, 6.9±0.6 cm, 7.5±0.6 cm, 7.0±0.5 cm, and 10.4±0.6 cm, respectively) than in females (5.1±0.5 cm, 6.4±0.5 cm, 7.0±0.5 cm, 6.5±0.5 cm, and 9.5±0.6 cm, respectively) (p<0.001). Circumference of IP of the thumb was significantly thicker in males (6.4±0.5 cm) than in females (5.9±0.5 cm) (p<0.001). The circumferences of PIP of the index finger, middle finger, and ring finger were significantly thicker in males (6.2±0.4 cm, 6.2±0.4 cm, and 5.8±0.4 cm, respectively) than in females (5.6±0.4 cm, 5.7±0.4 cm, and 5.3±0.3 cm, respectively) (p<0.001).
The circumference of the wrist was significantly thicker in males (16.7±1.0 cm) than in females (15.1±1.1 cm) (p<0.001). The width of the palm was significantly larger in males (8.8±0.5 cm) than in females (8.1±0.5 cm) (p<0.001). For the ratio of palm length/palm width, there was no significant difference between males and females (1.2±0.1 cm) (p=0.996).
FFF of the middle finger was significantly greater in males (17.9±6.6 N) than in females (8.6±3.9 N) (p<0.001). FEF of the index finger and ring finger were significantly greater in males (8.5±2.0 N and 7.1±2.2 N, respectively) than in females (5.3±1.7 N and 4.7±.8 N, respectively) (p<0.001).
Maximal force of exertion on grasping (GF) of fingers (from index finger to little finger), index finger, middle finger, and ring finger were significantly greater in males (458.9±95.9 N, 135.5±40.3 N, 139.6±45.9 N, and 101.8±41.7 N, respectively) than in females (245.6±69.2 N, 85.4±26.1 N, 85.9±26.7 N, and 68.1±21.9 N, respectively) (p<0.001) (Table 2).
For area, both palm area (p=0.579) and HSA (p=0.882) showed no difference between age groups. For length, the middle finger (p=0.008) differed in age groups, and post-hoc verification showed that the length of the middle finger in the 20s (7.4±0.6) was significantly longer than in the 60s (6.7±0.9). The length of the thumb (p=0.408), index finger (p=0.182), ring finger (p=0.538), and palm (p=0.488), excluding the middle finger, did not differ significantly in age groups. The thickness of PIP of the ring finger (p=0.018) was also found to have a significant difference between each age group, but post-validation by a Scheffé test showed no significant difference in the group.
For widths, there was no statistically significant difference between the age groups for palm (p=0.620) and palm length/palm width (p=0.314).
The FFF of the middle finger (p=0.537), FEF of the index finger (p=0.690), and FEF of the ring finger (p=0.061) showed no significant difference between age groups. GF of all fingers (p<0.001) had significant differences between each age group. Post-hoc analysis showed that GF of all fingers in participants in their 20s (411.8±155.8) was significantly larger than GF of all fingers in their 50s (268.55±78.54). The GF of the index finger (p=0.003) was statistically significant between each age group. Post-hoc analysis confirmed that GF of the index finger in people in their 20s was significantly greater than the GF of the index finger (84.1±29.1) of participants in their 40s. The GF of the middle finger had a significant difference between each age group (p=0.008), but no group had a significant difference in post-hoc verification by a Scheffé test (Table 3).
For males, the FFF prediction model by the circumference of the PIP joint of the middle finger (p=0.007) and the maximum force of the grasping force of the middle finger (p<0.001) were statistically significant. The explanatory power of the FFF prediction model for circumference of the PIP joint of the middle finger of the prediction model was about 13%, and the explanatory power of the FFF prediction model for the maximum force of the grasping force of the middle finger was confirmed to be about 22%.
For females, FFF prediction models by all variables, except the FFF prediction model for the circumference of the PIP joint of the middle finger, appeared to be statistically significant. The explanatory power of the predictive model depends on the variables, but it is about 9% to 30%. For males, the FFF prediction models by palm area and width were not statistically significant. In females, the FFF prediction model by the circumference of the PIP joint of the middle finger was not statistically significant.
Although there was a slight difference in trends, in both males and females, the middle finger has the highest explanatory power of the FFF prediction model due to the maximum force applied. Both the non-standardized coefficients and the standardized coefficients were positive, and all independent variables had a defining effect on FFF. In males, the area and width of the palm did not affect FFF, and GF had the highest explanatory power (Table 4).
For males, the predictive model by all independent variables except GF of the index finger, among the variables used to predict FEF, was not statistically significant. The predictive model by GF of the index finger was statistically significant with p=0.042, and the explanatory power of the predictive model was about 8%.
For females, as opposed to males, only the predictive model by GF of the index finger (p=0.062) was not statistically significant. Palm area (p=0.030), circumference of IP of the thumb (p=0.001), the circumference of the PIP of the index finger (p=0.001), the circumference of the wrist (p<0.001), the length of the index finger (p=0.034), HSA (p=0.004), palm length (p=0.007), and all prediction models by palm width (p=0.003) were statistically significant. The explanatory power of these models was about 7% to 18%. Among the statistically significant models, only the length of the index finger in females had negative coefficients, indicating that the shorter the length of the index finger, the greater the FEF (Table 5).
For males, the FEF prediction model of the ring finger by all independent variables was statistically significant: palm area (p=0.001), circumference of the wrist (p=0.018), circumference of PIP of the ring finger (p=0.014), circumference of IP of the thumb (p=0.001), HSA (p=0.005), and palm width (p=0.027). The explanatory power of these predictive models was found to be about 7% to 18%, but the prediction model for palm length (p=0.058) was not significant.
The predictive model for the palm area showed the highest explanatory power of 18.2%, but the constant value was 0.062, which had a defining effect but not a significant impact. The influence of the model by the circumference of the IP of the thumb was 17.8%, and the constant value was 1.919, indicating that the degree of influence was relatively large.
For females, the predictive model was statistically significant for the HSA (p=0.021) and palm length (p=0.028), while palm area, the circumference of the wrist, the circumference of the PIP of the ring finger, the circumference of the IP of the thumb, and palm width were highly significant (p<0.001). The explanatory power of the model was also relatively low for HSA (8.1%) and palm length (7.4%), and the explanatory power of the predictive model for all other variables was relatively high, ranging from 24.1% to a maximum of 36.7% (Table 6).
An analysis of the linear correlation between FEF and circumference and length confirmed that circumference had a stronger linear correlation than length. Therefore, linear regression was performed to develop a model that can predict FEF by the circumference of each finger.
The model where the FEF of the index finger=2.7×circumference of the index finger–9.52 was statistically significant (p<0.001), and the explanatory power of the predictive model was 28.5%.
The model for predicting the FEF of the middle finger by the circumference of the middle finger (FEF of the middle finger=7.727×circumference of the middle finger–33.025) was statistically significant (p<0.001), and the explanatory power of the predictive model was 27.9%. A model for the ring finger (FEF of the ring finger=2.975×circumference of the index finger–10.738) was statistically significant (p<0.001), and the explanatory power of the predictive model was 36.8% (Table 7).
Discussion
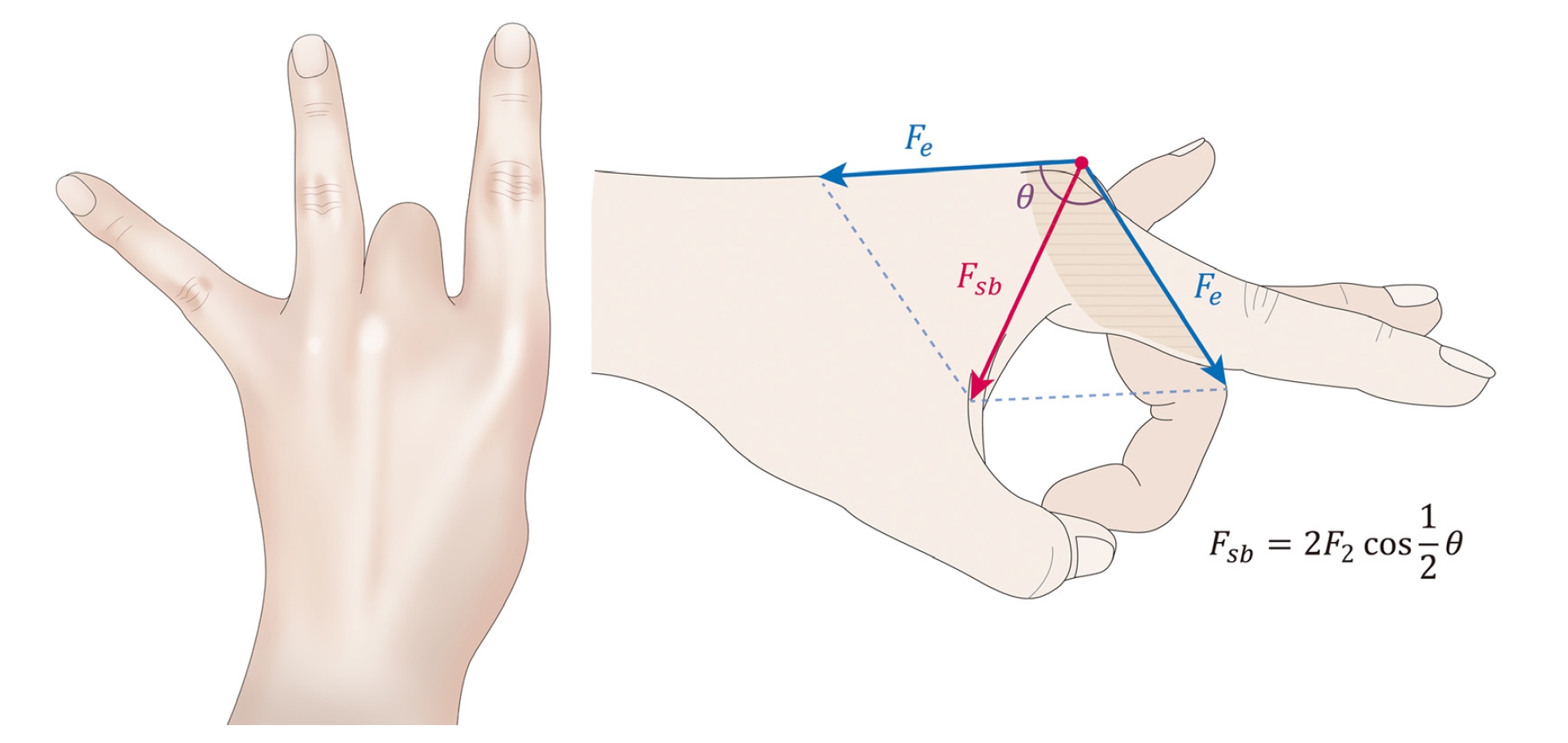
For the mechanism of force-generating during finger striking, Hong et al. [5] stated that when one tries to flick a finger harder, greater tension is exerted on the extensor tendon. In this situation, volar-ward force is generated on the extensor tendon over the bony prominence of the metacarpal head. If the extensor tendon is well aligned with the sagittal band and the extensor hood, not much force can be applied to the sagittal band. However, when the extensor tendon slips to either the radial or the ulnar side, the force applied to the sagittal band when it slips to the radial or ulnar side will be mainly exerted on the opposite side of the sagittal band (Fig. 3).
The nasal bones are the most fragile facial bones, with tolerance levels for minimal fractures ranging from 111.21 to 333.62 N. The maxilla has a low tolerance level (622.75–1,979.46 N). The zygomatic arch is relatively fragile (tolerance level, 925.23–2,112.91 N), while the zygomatic body has a higher tolerance level (889.64–2,001.70 N) [6]. Among the facial bones, fractures occurred at 111.21 to 333.62 N for the nasal bone, 622.75 to 1,979.46 N for the maxilla, 925.23 to 2,112.91 N for the zygomatic arch, and 889.64 to 2,001.70 N for the zygomatic body. The sizes of FEF (index finger, 6.8±2.5 N; ring finger, 5.8±2.3 N) and FFF (middle finger, 12.9±7.0 N) in this study were not sufficient to cause facial bone fractures (Table 2). Although finger striking is usually applied on the forehead, it might strike the nose if the finger is slipped by mistake.
The four independent variables related to size in this study had the greatest effects, which can be interpreted as indicating that there are factors other than the area or width of the palm that determine the size of this force. However, considering that the explanatory power was not very high (20%–30%), the possibility that there is an independent variable that has a greater effect on FFF than the independent variables selected for this study cannot be ruled out (Table 4).
The explanatory power of the FEF of the ring finger prediction model using the circumference of the PIP of the ring finger was the highest at 36.7%, and the constant value was also 3.136, indicating the greatest degree of influence (Table 6). Differences in bone thickness and muscle mass can determine the circumference of each finger, which seems to affect the FEF (N) and GF (N) (Table 7).
According to Langer et al. [7], the force exerted by the hand and fingers to apply pressure to an object was measured using a grip force meter. Ramakrishnan et al. [8] stated that palm thickness and width are strongly correlated with grip strength for all wrist postures, whether dominant or not. According to Balogun et al. [9], flexion and extension of the wrist and forearm rotation have important effects on grip strength and interact with grip strength along with elbow posture. Fransson and Winkel [10] stated that grip strength is absolutely related to hand size. It turns out that females’ lower grip strength is due to their hands being smaller than those of males. According to Kim et al. [11], most of the muscles that make up the forearm are related to the movements of the wrist and fingers. In order to identify the correlation between the movement and the electromyographic signal generated through the motion of gripping the fingers, learning data that could simultaneously estimate the strength of the wrist and the grip strength were constructed [11].
When the index finger and ring finger were compared with the independent sample t-test, the FEF, girth, and grip force values of the index finger were statistically significantly greater than that of the ring finger. However, there was no significant difference in length between the index and ring fingers (Table 8).
According to Hong et al. [5], subluxation occurs most frequently in long fingers. However, comparing the index and ring fingers in this study, there was no difference in length, but the FEF, finger circumference, and grip strength were greater in the index finger. Therefore, the size of the FEF is more closely related to the finger circumference and grip strength than the finger length when taking the finger-striking posture.
Chauhan et al. [12] reviewed hand injuries according to zone and stated that zone V injury is a sagittal band rupture that may result from blunt trauma to the metacarpophalangeal (MCP) joint, a laceration or direct injury to the sagittal band, and resistance to extension or flexion across the MCP joint. This injury type is also referred to as “boxer’s knuckle” because these injuries frequently occur in athletes in direct contact (i.e., in boxing, soccer, and rugby).
ElMaraghy et al. [13] wrote that subluxation most often occurs in the middle finger. The middle finger has the anatomical features of a long radial sagittal band, a prominent metacarpal head, a rounded cross-section of the extensor tendon, increased distal extension of the sagittal band, and less substantial juncturae tendinum compared to the ring and little fingers.
Hong et al. [5] reported 26 cases of extensor tendon subluxation due to the finger striking posture. In all patients, the damaged area was the long finger, which was subluxed to the ulnar side, and slipping of the extensor tendon during finger striking frequently occurred on the long finger and ulnar side.
Beck et al. [14] reported that in two extensor tendon dislocation patients, the middle finger’s extensor tendon was exposed, and the fibers attached to the extensor hood were few, so the dislocation occurred most in the middle finger extensor tendon.
Young and Rayan [15] dissected to investigate the mechanism of sagittal band damage in the hands of 10 frozen cadavers and two fixed cadavers. The authors said that when the MCP is fully flexed during trauma, it is vulnerable to collateral ligament damage. When accompanied by wrist flexion, this force can be increased and the injury can be aggravated.
Rayan and Murray [16] classified sagittal band injuries into three types as follows: mild injuries without instability were classified as type I, moderate injuries with extensor tendon subluxation, type II, and severe injuries with tendon dislocation, type III.
Peelman et al. [17] treated 92 patients who complained of sagittal band incompetence by applying the following two types of splints: first, a “P-blocker splint” that is applied to the hand or forearm to prevent bending of the MCP; and second, a “sagittal band bridge splint” that restricts the bending of the MCP joint in the sphenoid region by hanging on both sides of the finger. The authors reported that splint therapy was very effective in acute sagittal band incompetence.
As a surgical method to reconstruct the ruptured sagittal band, there is a method of reattaching the superficial layer of the ruptured sagittal band to the outside of the extensor tendon5 by making a slip and loop with the accessory extensor tendon and fixing it in the middle of the extensor digitorum communis [14].
Kang et al. [18] recommended primary suture in case of acute dislocation of the extensor tendon, and for chronic cases, reconstruction using part of the soft tissue, accessory tendon, extensor tendon, etc. around the wound site was suggested.
This study has two limitations. First, the design did not account for the anatomic complexity of the index finger, specifically the independent extension capability mediated by the extensor indicis proprius muscle. This factor, along with finger circumference and grip strength, could influence the results. Second, a biomechanical limitation exists as the study did not measure the flexion angle at the MCP joint during the flicking motion (flick angle). The flick angle influences the force applied to the sagittal band upon slippage, potentially affecting the risk of extensor tendon subluxation. These limitations highlight the need for further studies that incorporate both anatomical considerations and the biomechanics of the flicking motion to obtain a more comprehensive understanding of extensor tendon subluxation.
Conclusion
As all characteristics increased, the FEF of the middle finger, the FFF of the index finger, and the FEF of the ring finger also tended to increase. It was confirmed that the index finger’s measurement average was linearly correlated with the index finger’s circumference (ρ=0.533), the middle finger’s measurement average was linearly correlated with the middle finger’s circumference (ρ=0.528), and the ring finger’s measurement average was linearly correlated with the ring finger’s circumference (ρ=0.60). The results of this study will help to understand the relationship between the forces generated in the process of finger flicking through the anatomical measurements of the hand.