Surgical treatment of high-pressure injection injuries of the hand caused by using paint guns: a report of three serial cases
Article information

Abstract
The incidence of high-pressure injection injuries is increasing with the development of industry and use of injectors. Although high-pressure injection injuries are relatively rare, they commonly lead to complications such as skin necrosis, infection, and amputation. Moreover, the initial presentation is prone to be underestimated because of the small entry point at the patient’s first encounter in emergency care. A prompt surgical intervention is required, with appropriate and rapid initial treatments, including broad-spectrum antibiotics and tetanus toxoid. The surgical treatment involves wide debridement for foreign material removal and subsequent reconstruction. In this case report, we present three cases we encountered and the ensuing complications. All three patients who received the same treatments are discussed in detail.
Introduction
High-pressure injection injury is relatively rare, but it can lead to severe consequences such as soft tissue necrosis, infection, and eventual amputation, all of which result in functional impairment [1,2]. The incidence of high-pressure paint gun injection injury is increasing with the development of industry and the increase in the use of paint guns [3]. High-pressure paint gun can produce pressure from 2000 up to 12,000 pounds per square inch (psi). Devastating injuries can be expected from these traumas, considering that a pressure of 100 psi is sufficient to breach the skin surface [2]. The most commonly injected materials are paint and grease, but also include paint solvents, fuel oil, water, air, and even animal vaccines [4]. The injury usually occurs on the non-dominant hand because the injection device is held by the dominant hand [4,5]. High-pressure paint gun injuries are initially treated with administration of broad-spectrum antibiotics and tetanus toxoid, while surgical intervention, including wide debridement, should be performed promptly after appropriate initial evaluation and management. Here, we present three cases of high-pressure injection injury by paint gun, which were treated at our institution, and conducted an in-depth review of relevant literature.
Case report
This report was approved from the Institutional Review Board of Kangdong Sacred Heart Hospital (No. KANGDONG 2022-10-022). Written informed consent was obtained from all the patient for the publication of this report including all clinical images.
1. Case 1
A 59-year-old man with no underlying disease visited the emergency department for penetration injury of the left palm caused by paint gun injection (Table 1). A small entry port with minor swelling and redness was noted from the initial examination (Fig. 1A). Computed tomography (CT) imaging workups of the left hand showed a 1×1 cm-sized foreign material located in the soft tissue above the flexor tendon sheath (Fig. 1B, 1C). Surgical debridement and foreign material removal were sequentially performed 2 days after injury. Unfortunately, through Bruner’s incision, the emulsion paint was shown to strongly adhere to the surrounding structures such as the lumbrical muscles, common digital nerves from the median nerve, and even to the skin and fat layers (Fig. 1D). Inspection revealed partial injury to the tendon sheath, while the tendon itself was preserved. Meticulous dissection and skeletonization of the affected structures were necessary. After copious irrigation, the surgical wound was closed by placing a Penrose drain (Fig. 1E). During daily observation, the drain was removed on postoperative day 2. In addition, wound culture revealed no pathogen presence. Accordingly, the approximated wound showed satisfactory progress, and the patient was discharged 4 days after surgical intervention. The wound and function of the hand including flexion and extension were completely healed without any infection, necrosis, or limitation of motion (Fig. 1F).
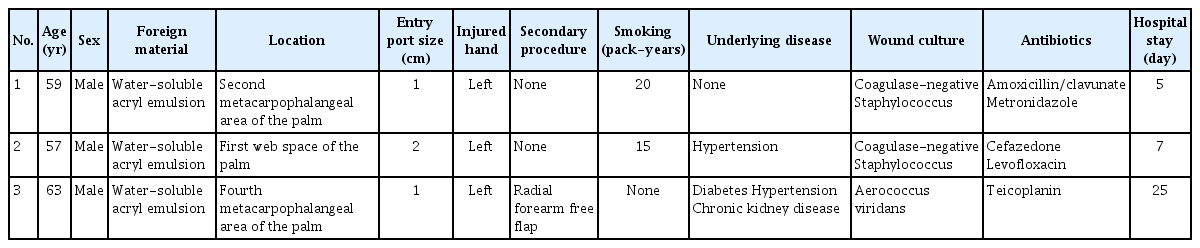
The demographic and clinical characteristics of three patients who had high-pressure injection injuries
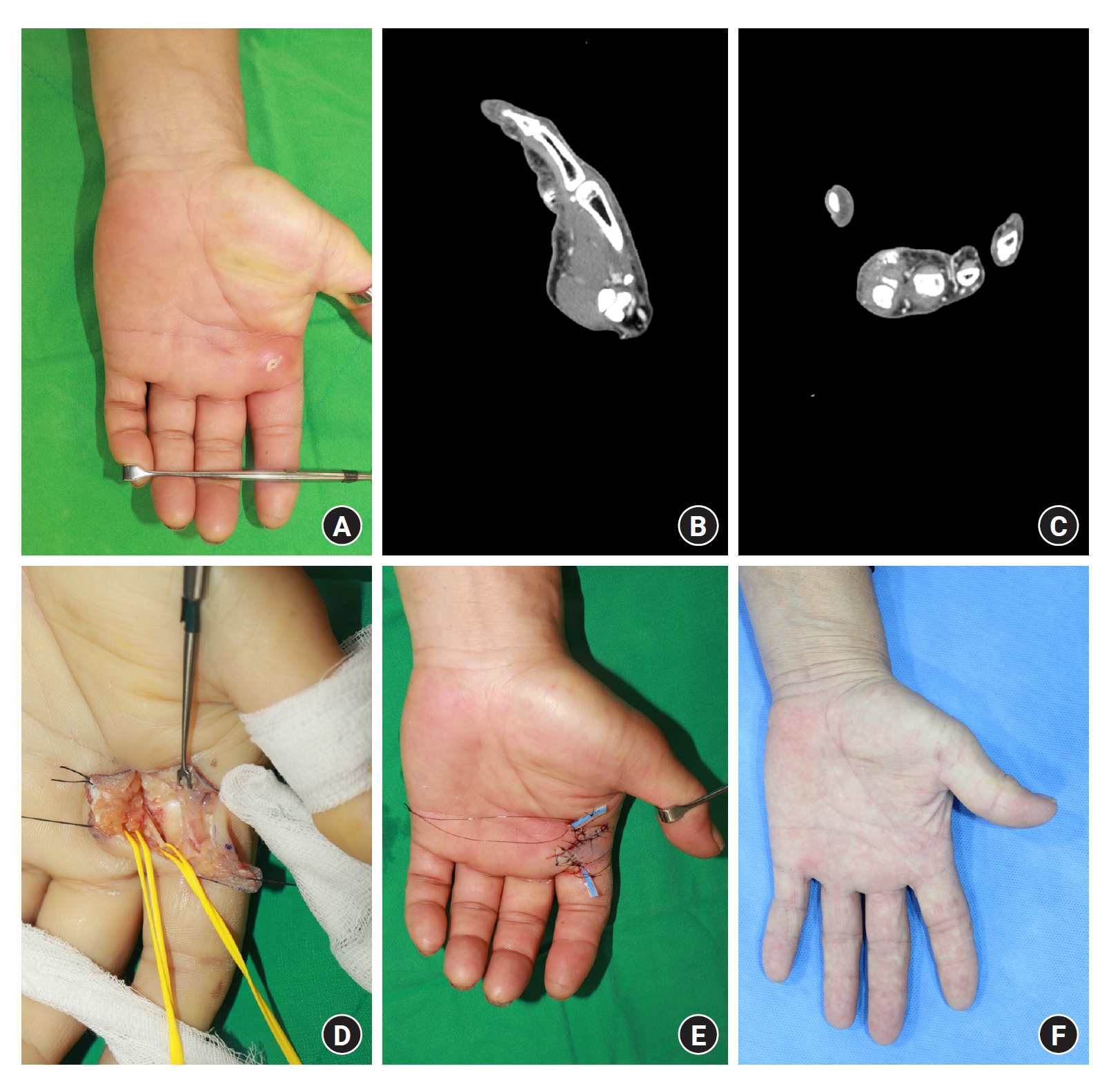
A 59-year-old man visited with a high-pressure paint gun injury on his left hand. (A) A preoperative photograph shows a small entry point at the second metacarpophalangeal level. (B, C) Preoperative images. Computed tomography images show a 1-cm foreign body in the palmar aspect of the metacarpophalangeal joint level (B, sagittal view; C, axial view). (D) An intraoperative photograph shows that the paint adhered to soft tissues. (E, F) Postoperative photographs. (E) The wound was sutured with a drain insertion. (F) A postoperative photograph shows completely healed wound, with no complications, and the patient exhibited almost complete recovery in his hand function at 6 months after the operation.
2. Case 2
A 57-year-old male with hypertension suffered an injury to his left palm by a high-pressure injection gun (Table 1). The high-pressure water-soluble acryl emulsion paint penetrated the skin of the first web space (Fig. 2A). From the first inspection, the entry port was approximately 0.5 cm in size, and minor swelling and redness were noted. The patient complained of pain and tenderness, although no limitations of motor function and sensory impairment were observed. Wide spreading of the radiopaque lesion (considered as the foreign material) across the dorsal area of the hand was verified in the X-ray imaging test (Fig. 2B). The patient immediately received broad-spectrum antibiotics before undergoing surgery, including exploration and wide debridement, 5 hours after injury. Similar to the first case, the emulsion material was found to be strongly adhered to the first dorsal metacarpal artery and deep fascia; thus, debridement with skeletonization for nerves or vessels was performed under a microscope. Following the extension incision to the dorsal area, the same procedure was repeated for the accumulated material (Fig. 2C). No nerve or vessel injury was identified. Gentle closure of the wound after copious irrigation was performed, and the wound culture test showed normal skin flora. The patient returned home on the 7th day of hospitalization. His hand function was almost restored sufficiently for him to return to work. The patient reported no distinct discomfort throughout the 6 months of observation (Fig. 2D).

A 57-year-old man who had hypertension injured his left hand by a high-pressure paint gun. (A) A preoperative photograph. Entries are shown on the left palm of the hand, first web space area, and third metacarpophalangeal area. (B) An X-ray image of the left hand. Radiopaque lesions considered as foreign bodies are seen in the first web space area. (C) An intraoperative photograph during the radical debridement with extended incisions. The whitish paint materials are seen adhering to the muscles and tendons. (D) A postoperative photograph a month after the operation. The wound had healed without any complication.
3. Case 3
A 63-year-old male with diabetes, hypertension, and chronic kidney disease injured his left palm using a high-pressure injection gun (Fig. 3A, Table 1). CT scanning showed that the injected material spread through the palm and even the hand dorsum (Fig. 3B, 3C). Worse still, the radiopaque material was widespread to the third and fourth metacarpal area of the left palmar and dorsal hands. Initially, the patient was referred to an orthopedic surgeon on duty. After surgical exploration and debridement, he was subsequently transferred to the plastic surgery department for further debridement, removal of residual foreign bodies, and reconstruction. Prior to the reconstructive procedure, another wide debridement involving radical dissection of the surrounding structures was conducted (Fig. 3D). The infiltration of the emulsion paint into the skin and adipose layers was extensive, and wide resection of the volar skin envelope, including the entry port, was required. Subsequently, sequential flap reconstruction for soft tissue coverage was continued. A radial forearm flap from the contralateral side was chosen to cover the same defect; this flap was designed as a 3.5×10-cm elliptic shape with a long tail to ensure the anastomosis site from the injury zone of the palm. Consequently, the flap was raised and transferred to the defect with end-to-side anastomosis to the radial artery near the wrist and end-to-end anastomosis to the vena comminates and superficial branch of the cephalic vein. The flap settled into the area gradually, and rehabilitation therapy has begun. The flap debulking procedure with minor revision is ongoing to facilitate hand function, and his hand function was recovered up to 90° of flexion at the proximal interphalangeal joint and 30° of flexion at the distal interphalangeal joint at his 9-month follow-up (Fig. 3E, 3F, 3G). Furthermore, the patient was also able to perform activities such as grasping a cup.

A 63-year-old man with a high-pressure paint gun injury was referred from the Department of Orthopedics. (A) A 1-cm wound surrounded by a blackish area. (B, C) The injected paint is seen penetrating to the dorsal side of the hand. (D) An intraoperative photograph shows the arteries, nerves, and tendons that were dissected and located in the injury zone. (E–G) Photographs taken 9 months postoperative. (E) The palmar side of the hand shows a well-taken flap after a debulking procedure. (F) The dorsal side of the hand recovered with no complications. (G) The injured ring finger demonstrated functional recovery up to 90° of flexion at the proximal interphalangeal joint and 30° of flexion at the distal interphalangeal joint.
Discussion
Since the first high-pressure injection injury by paint gun was reported in 1963, the incidence of these injuries has increased with the development of techniques and industry [6]. According to Verhoeven and Hierner [7], one in every 600 hand traumas relates to high-pressure injection injury, and one to four people visit large-scale hospitals for similar injection traumas per year. The number of male patients (70.7%) is more than double that of female patients (29.3%) [4]. Moreover, some studies have reported that the index finger was the most common location of injection injury to the hand, followed by the middle finger and palm [2,4].
Paint and grease are commonly used in high-pressure hand tools, although other materials, such as solvent, fuel oil, cement, water, air, and even animal vaccines, can also be used in these tools. It is important to identify the injected material because it can affect the progress from the surgical debridement and healing stages [2,4]. For instance, injuries from organic solvents have a higher amputation rate (>40%) [2,4]. The intense inflammatory response that promotes vasospasm and rapid tissue necrosis is considered to be the main mechanism of poor prognosis. Primary amputation can also be proposed to deal with paint injection injuries [2]. Indeed, the injection pressure is correlated with the amputation rate. According to Schoo et al. [8], the amputation rate increases when the injection pressure is more than 1,000 psi, but there is no pressure threshold for which amputation is inevitable. However, Verhoeven and Hierner [7] reported that when the pressure is >7,100 psi, the amputation rate is 100%. Therefore, more specific questions about the paint gun’s injection pressure and even requesting for paint gun what the patient used are needed, because patients rarely remember or know their paint gun’s injection pressure.
Sequential tests should be conducted based on this information. Imaging findings are important to confirm the extent of injected materials before surgical intervention, while X-ray or CT can detect injected material according to the content of radiopaque leads [5].
The timing of surgical intervention is the most critical factor affecting the prognosis of high-pressure injection injury [1,2,4]. Wide surgical debridement should be performed in the early stage to deal with compartmental pressure, inflammatory responses, and infections [2,4]. The amputation rate has been reported as 40% when surgical debridement was completed within 6 hours, but increased when exceeding 6 hours, reaching up to 88% when surgery was delayed for more than a week [4]. Surgical repair of defects after wide debridement is also important and can be performed using various methods, from direct closure to tissue transfer, depending on the defect size and status. Moreover, proper selection of the recipient vessel is essential for successful free flap transfer. To the best of our knowledge, the cause of failure was the proximity of the anastomosis to the injury zone. Recipient vessels should be sufficiently far from the zone of injury. The potentially traumatized recipients that are close or even near surroundings to the zone of injury can cause poor blood supply to the flap.
Inflammation of the tendon can cause adhesions and severe functional impairment, even in instances where primary removal of the injected material and surgical repair are performed. The average motion limits are 8° at the metacarpophalangeal joint, 24° at the proximal interphalangeal joint, and 30° at the distal interphalangeal joint [4]. Therefore, sequential adhesiolysis or revision of tendons may be required following the primary procedure. Without doubt, rehabilitation management should be continued for improved hand function.
Here, we present three cases of high-pressure gun injury in males with water-soluble acryl paint injuries to the non-dominant hands. None of the patients underwent amputation, but flap failure was observed in a single case because of poor blood supply to the transferred flap, which was finally replaced with another free flap. These injuries are likely to be missed due to minor symptoms and relatively small wound sizes, which delays the timing of proper surgical intervention and can have fatal consequences. For these reasons, we report our experiences to contribute to the appropriate and satisfactory treatment of this condition.
Notes
The authors have nothing to disclose.
Funding
None.