



Introduction
Humerus shaft fractures account for about 1% to 3% of all fractures, and approximately 20% of humerus fractures [1-3]. According to previous studies, the incidence of humeral shaft fractures in the general population shows a bimodal age distribution, with injury occurring more frequently in those under 30 and over 60 years old [4-7]. The most common cause of humeral shaft fractures in elderly individuals is a simple fall, with osteoporosis believed to be a risk factor. In the younger age group, high-energy injuries such as traffic accidents were identified as the main cause, followed by falls [4,8].
Several studies have reported traumatic humeral shaft fractures in soldiers, the majority of whom are young adults. In a prior study, Chao et al. [9] reported on 129 patients with humeral shaft fractures that occurred during grenade-throwing practice. They reported that conservative treatment using a hanging cast was performed in all cases, and surgical treatment was subsequently performed in only three patients with persistent radial nerve palsy. Pehlivan et al. [10] also reported on 27 patients with humeral shaft fractures that occurred during grenade-throwing practice; in this cohort, all patients were treated with a functional brace, and no patients showed neurological symptoms. In a recent study of 123 cases of humeral shaft fractures in Korean soldiers, the most common cause was arm wrestling (65 cases, 52.8%), and most patients were treated with surgery at Armed Forces Capital Hospital [11]. However, their research has the limitation that they cannot represent the entire Korean military in all regions.
Therefore, the purpose of the present study was to investigate the epidemiological features and surgical results of traumatic humeral shaft fractures in a group of young adults in the Korean military at other military hospitals in other regions.
Methods
This study was approved by the Institutional Review Board of Armed Forces Daejeon Hospital (No. AFMC-202203-HR-014-01). Written informed consent was obtained from the patient for the publication of all clinical images.
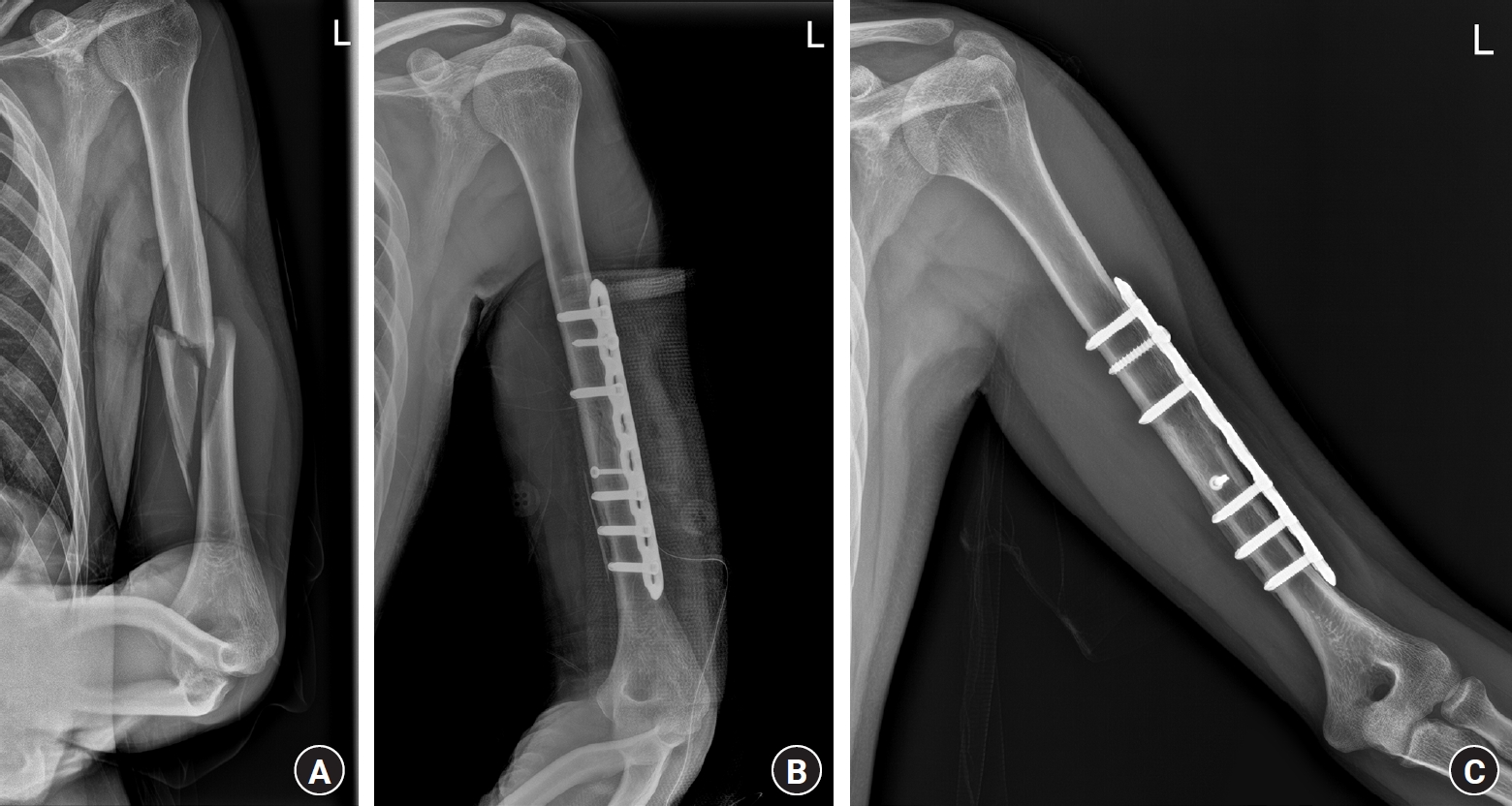
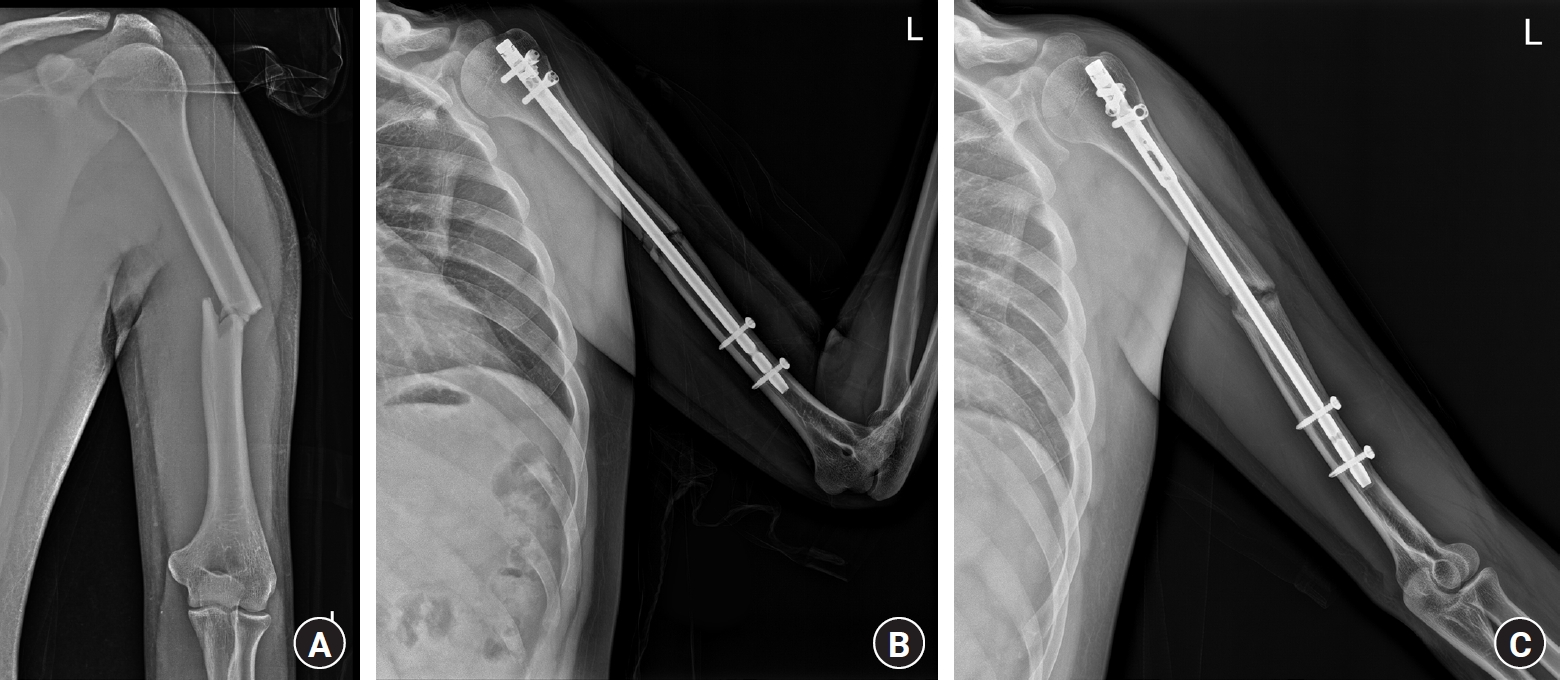
We reviewed the medical records of patients who visited the outpatient clinic or emergency department of Armed Forces Daejeon Hospital between May 2019 and October 2021. All patients diagnosed with traumatic humeral shaft fractures after entering the military service were included in this study. Humeral shaft fracture was defined as a fracture occurring between the superior border of the insertion of the pectoralis major and the area immediately above the supracondylar ridge, in accordance with the definition of Tytherleigh-Strong et al. [6]. Patients with accompanying injuries to the ipsilateral upper limb were excluded. No open fractures or pathological fractures were observed. The patients included in this study were active young soldiers, all of whom underwent surgical treatment to expedite their return to duty. Some patients visited our hospital for hospitalization after surgical treatment at another hospital, and some patients underwent surgery at our hospital. Surgical treatment included internal fixation using plates and screws or intramedullary nailing (Figs. 1–3). Demographic and clinical data including age, sex, body mass index (BMI), smoking status, injury mechanism, fracture pattern, and manifestation of radial nerve palsy were collected and analyzed, and fracture patterns were classified according to the Orthopaedic Trauma Association (OTA) system [12]. The mechanism of injury was classified as a fall from a height, sports-related slip, arm wrestling, rope-related training, or miscellaneous (e.g., operating the machine and one-hand push-ups). For patients who underwent surgery at our hospital and were followed up as outpatients, we additionally investigated time to union, follow-up period, Disability of the Arm, Shoulder, and Hand questionnaire (DASH), visual analog scale (VAS) score for pain at the final follow-up, and the occurrence of complications.
The Student t-test was used for comparison of normally distributed dependent continuous variables, while the Mann-Whitney U-test was used for inter-group comparisons of nonnormally distributed dependent, continuous, or sequential variables. In addition, when the dependent variable was a nominal variable, the chi-square test was used, and when the expected frequency was less than five cells in 20% or more, the Fisher exact test was used.
Results
A total of 31 patients with traumatic humeral shaft fractures were included in this study. The demographic data of the study cohort are shown in Table 1. The average age was 22.03±1.56 years, and all patients were male. The mean BMI was 23.18±1.73 kg/m2, and 11 patients (35.5%) were current or former smokers. Arm wrestling (17 patients, 54.8%) was the most common cause of fracture, followed by rope-related training (five patients, 16.1%), and falling from a height (four patients, 12.9%). According to the OTA Classification, 14 patients had 12-A1 simple spiral fracture (45.2%), one patient had 12-A3 simple transverse fracture (3.2%), 15 patients had 12-B1 wedge spiral fracture (48.4%), and one patient had 12-C1 complex spiral fracture (3.2%). All 12-B1 wedge spiral fractures showed a medial butterfly wedge fragment pattern. Thirty of the 31 patients had a spiral fracture (96.8%), and one had a transverse fracture (3.2%). Regarding location, 16 were distal fractures (51.6%) and 15 were middle fractures (48.4%). Radial nerve palsy was present in nine patients (29.0%). The patients were divided into arm wrestling (n=17) and other groups (n=14), and the characteristics of the fractures were compared. We identified a difference in the proportion of fracture types and locations; however, this difference was not statistically significant (Table 2). Patients were able to return to simple daily activities within 2 weeks after surgery. Three months after surgery, most patients were able to return to work, including exercise and training. There were 14 patients who underwent surgery at our military hospital, and the average outpatient follow-up period was 13.21±4.63 months and the mean time to bone union was 12.08±1.32 weeks (Table 3). At the final follow-up, the DASH score was 11.01±13.51, and the VAS score for pain was 2.29±1.20. Radial nerve palsy symptoms occurred in two patients (14.3%), and they fully recovered after 8 weeks and 5 months, respectively. There was one case of nonunion using intramedullary nailing, and it was determined that atrophic nonunion occurred because the fracture site was distracted and fixed (Fig. 3).
Discussion
We investigated the causes and treatment outcomes of humeral shaft fractures in young soldiers in South Korea. Arm wrestling was the most common cause of fracture in 17 of the 31 patients included in the study, accounting for approximately 54% of all patients. The next most common causes were rope-related training and falling from a height. There were no statistically significant differences in fracture patterns and complications between the arm-wrestling group and the other groups. The average bone union time of patients who underwent surgery at our hospital was approximately 12 weeks, and the average DASH score at the final follow-up was 11 points, indicating satisfactory results. However, radial nerve palsy symptoms were higher than normal and occurred in approximately 14% of patients.
Arm wrestling is a rare cause of humeral shaft fractures in the general population. Mattila et al. [1] previously reported humeral shaft fractures in 936 patients treated at Helsinki University Hospital, of which only 31 (3.3%) were due to arm wrestling. In addition, Mayfield and Egol [13] analyzed 93 patients with humeral shaft fractures, and only 9 of fractures (9.7%) were caused by arm wrestling. However, in a study of humeral shaft fractures in Korean soldiers, Kim et al. [11] reported that approximately 53% (65 of 123) of the patients were injured during arm wrestling. The timing of the study and the service area of the patients were different from Kim et al.’s study [11], similar results were obtained in our study. Therefore, this study is meaningful in supporting the fact that arm wrestling is the most common cause of humerus fractures in Korean soldiers. We did not clarify why arm wrestling was the most common cause of humeral fractures among Korean soldiers. However, assuming the reason, the soldiers were mostly males in their 20s, and compared to the general population, arm wrestling would have been practiced more commonly as a form of entertainment. Thus, as the number of practice sessions was greater, the soldiers would have been at greater risk of injury. Therefore, to reduce the damage caused by arm wrestling, it is necessary to educate soldiers about the dangers of arm wrestling and refrain from arm wrestling in the barracks.
Several studies have previously investigated the pathogenesis of humeral shaft fractures during arm wrestling. Moon et al. [14] suggested that the rotatory force and accompanying axial load are the mechanisms responsible for the occurrence of humeral shaft spiral fractures with butterfly fragments. Ogawa and Ui [15] further reported that fractures occur when the internal rotator muscles of the shoulder suddenly shift from maximal concentric contraction to eccentric contraction due to a weight shift. At this time, it was estimated that eccentric contraction would be further strengthened by the counteraction of the arm wrestler’s opponent, eventually leading to fractures. Mayfield and Egol [13] reported that arm-wrestling participants experienced fractures while trying to counteract the increased external rotational force on the arm by their opponent. In other words, the pectoralis major, latissimus dorsi, teres major, and subscapularis generate internal rotational forces in response to the external rotational force reinforced by their opponent. This opposing force acts as a lever on the humerus, strengthening the eccentric contraction and causing humeral fracture. According to a previous biomechanical study, the bone mineral density of the mid-to-distal-third area of the humerus is lower than that of other parts, and the ratio of the outer diameter to the inner diameter is small; therefore, fractures occur easily in that area during arm wrestling [16]. In our study, most fractures were mid-to-distal spiral fractures, and the proportion of fractures with medial butterfly fragments reached approximately 48%.
The incidence of radial nerve palsy associated with humeral shaft fractures is approximately 10% of the general population [1,17]. In Holstein-Lewis fractures, which are known to cause radial nerve palsy more often, this rate rises to approximately 20% [18-20]. Risk factors for radial nerve palsy in humeral shaft fractures have been identified as fractures in the mid to distal portion, spiral-type fractures, and high-energy trauma [2,21]. In our study, the incidence of radial nerve palsy was 29%, which is approximately twice as high as that in the general population. Considering this, all fractures occurred in the mid-to-distal portion, and most fractures were of the spiral type. In other words, most participants included in the study had risk factors for the location and pattern of fractures. However, most patients experience fractures due to low-energy trauma, which is not the risk factor for radial nerve palsy.
This study had several limitations. The small number of patients included in the study and the fact that this was a retrospective observational study, rather than a prospective study may have introduced bias and limits the generalizability of the results. Additionally, because not all military patients visited the authors’ hospitals, our results may not necessarily represent all military patients.
Conclusion
Arm wrestling is the most common cause of humeral shaft fractures among soldiers in South Korea. In this study, we found no significant differences in the patterns of humeral shaft fractures caused by arm wrestling and those caused by other causes, and the results of surgical treatment were good.