



Introduction
Lymphedema is a chronic disease that affects patients’ quality of life. The incidence of breast cancer-related lymphedema ranges from 6% to 30% [1,2]. There is currently no gold standard treatment for the disease, but numerous methods are being investigated. One treatment option is vascularized groin lymph node transfer (VGLNT), which replenishes lymphatic drainage in the affected area with transplanted intact lymph nodes sourced from another area [3,4]. Detailed knowledge of the superficial inguinal lymph node (SILN) anatomy is essential for a successful operation without complications.
To date, SILNs are known to be concentrated 3 cm perpendicular to one-third of the line from the pubic tubercle (PT) toward the anterior superior iliac spine (ASIS) [3,5]. However, no studies have compared the lymph node anatomy between patients and individuals without lymphedema.
Various factors, including obesity, radiation, postoperative infection, and genetic factors, increase the risk of lymphedema [6,7]. We hypothesized that these risk factors could affect the donor-site lymph nodes and impede the outcome of lymph node transfer surgery. This surgery will be problematic if the patient’s donor-site lymph nodes are insufficient when VGLNT is planned. Therefore, this study aimed to study the anatomy of SILNs and compare it between patients with lymphedema and individuals without lymphedema. In addition, computed tomography (CT) is a widely used, cost-effective, and accessible tool for studying the anatomy of SILN [8,9]. Therefore, we tried to investigate the applicability of CT for the preoperative planning of VGLNT.
Methods
Ethics statement: The study protocol was approved by the Institutional Review Board of Korea University Ansan Hospital (No. 2021AS0150). This study was performed in accordance with the Declaration of Helsinki and written informed consent was waived due to its retrospective nature.
1. Patients
This study retrospectively analyzed patients with upper-extremity lymphedema who underwent VGLNT from January 2015 to December 2020 by a single surgeon (DWK). Eighty patients with lymphedema who visited the Korea University Ansan Hospital were included. Patients who had upper-extremity lymphedema after breast cancer surgery and had undergone a preoperative contrast-enhanced pelvic CT were included. Patients with a history of other cancers and inguinal operations were excluded. Patients with a history of postoperative infection after breast surgery were also excluded because it is a known risk factor for lymphedema and could have affected our results [6].
After applying the inclusion and exclusion criteria, 17 patients with upper-extremity lymphedema were included. Thirty-four controls were selected as the normal group from the healthy individuals who had pelvic CT for regular medical checkups without related diagnosis and lymphedema and had characteristics similar to the patient group. For an accurate comparison, we have matched age, body mass index (BMI), and smoking history between the patient group and the normal group.
2. Methods
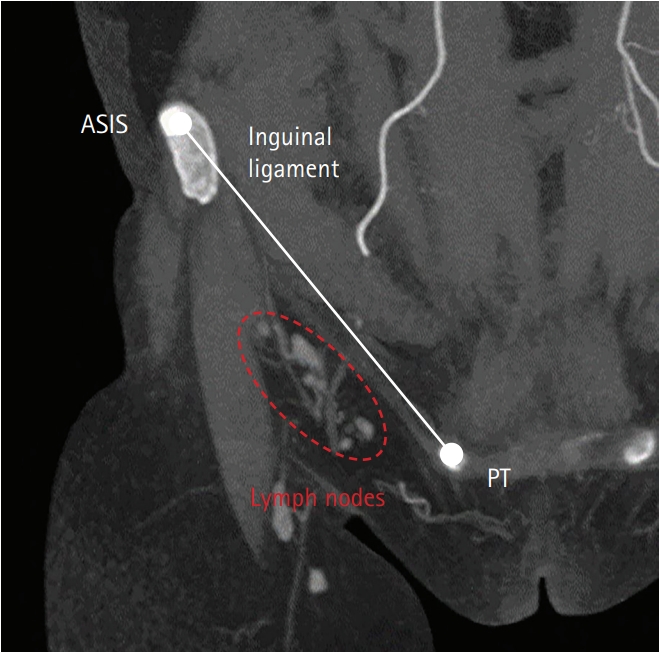
After the patients with lymphedema (comprising the patient group) and individuals without lymphedema (comprising the normal group) were selected, their CT scan results were evaluated. First, the number of lymph nodes was counted. On the coronal view, a line was drawn between the ASIS and PT, which coincided with the inguinal ligament. The SILNs inferior to the inguinal ligament were counted and marked (Fig. 1). Deep inguinal lymph nodes were excluded since VGLNT only harvests the SILNs.
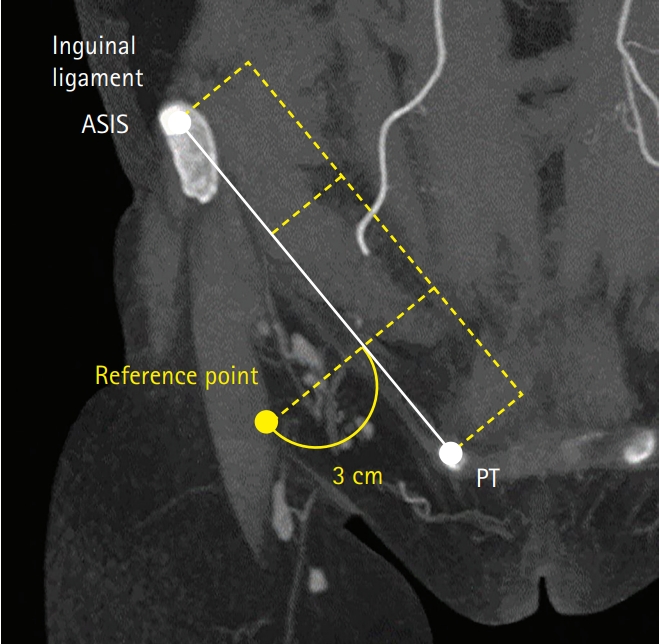
A reference point was marked 3 cm perpendicularly below one-third of the line from the PT toward the ASIS (Fig. 2). The distribution of lymph nodes was measured in two ways: by estimating the distance of the lymph nodes from the reference point and calculating the percentage of lymph nodes within the 3-cm boundary from the reference point.
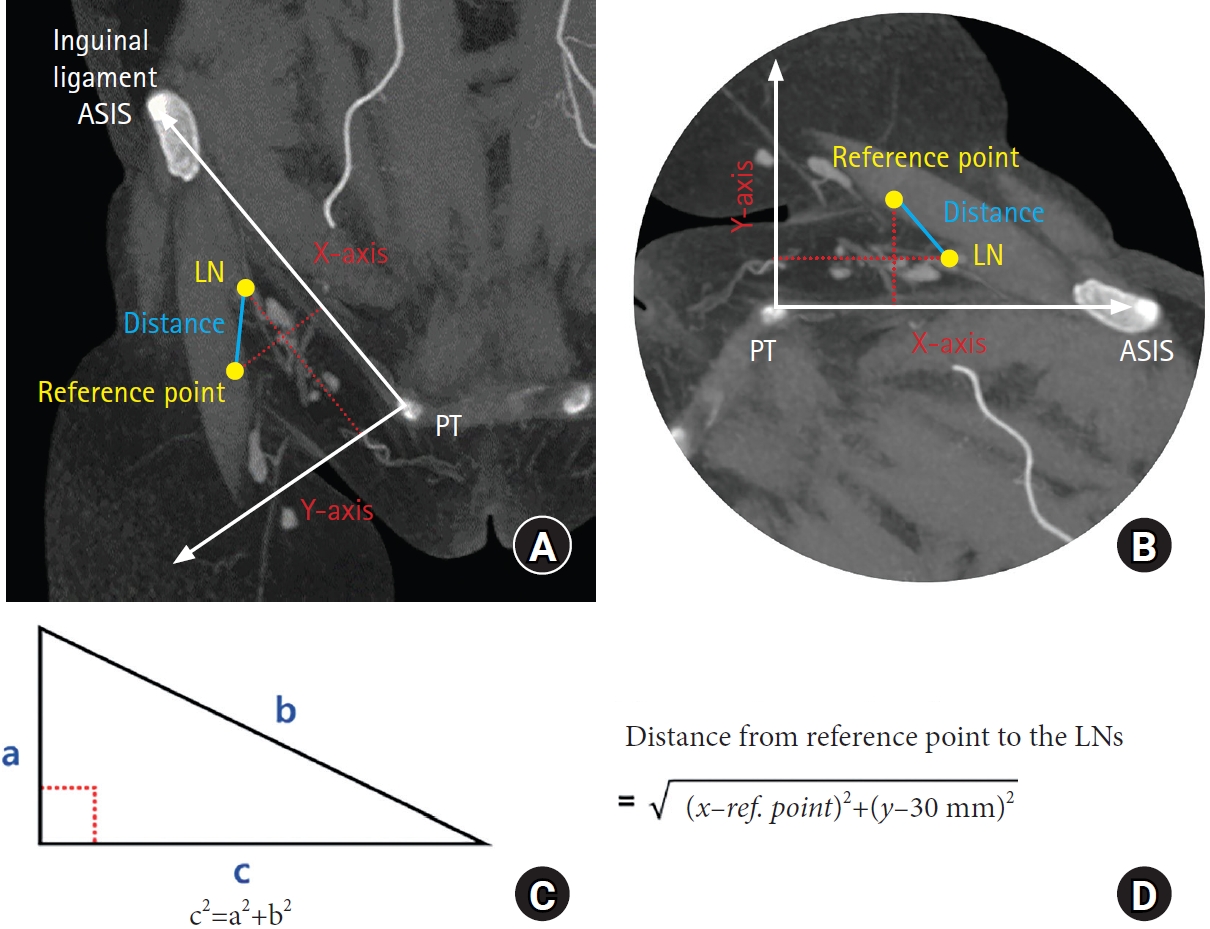
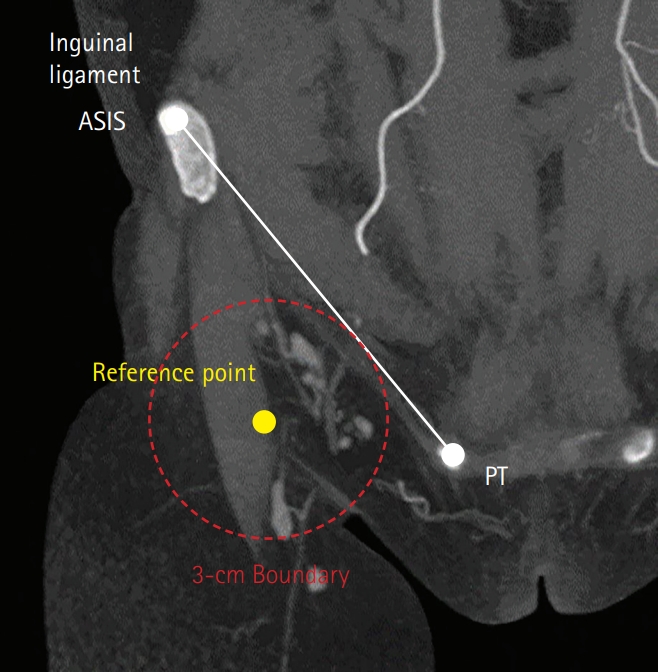
The coordinates of each lymph node were obtained by defining the inguinal ligament line as the ‘X’ axis and a line perpendicular to this as the ‘Y’ axis (Fig. 3A). The length of ‘b’ was calculated by subtracting the distance of the reference point from the X axis. Similarly, the length of ‘a’ was calculated by subtracting the value of coordinates of the SILN on the Y axis from 30 mm. Using the Pythagorean theory, the length of ‘c,’ which is the distance from the reference point to the lymph node, was calculated (Fig. 3B–3D). Based on the calculated distance, the percentage of lymph nodes within the 3-cm boundary from the reference point was obtained (Fig. 4). Two investigators independently interpreted the CT images for the landmarks, the reference point, and SILNs. The mean of their measurements was expressed as mean±standard deviation.
3. Statistical analysis
The normality test results were unsatisfactory because of the small number of patients. Hence, the Mann-Whitney U-test was used to compare the number of lymph nodes and their distance from the reference point between groups. The chi-square test was used to compare the percentage of lymph nodes within the 3-cm boundary of the reference point between the groups. The following statistical tests were used to compare patient characteristic variables between the groups: the t-test for age, the Mann-Whitney test for BMI, the Fisher exact test for smoking, and the Pearson chi-square test for chemotherapy history. All statistical analyses were conducted using the SPSS software ver.10 (SPSS Inc., Chicago, IL, USA). The level of statistical significance was set at p<0.05.
Results
We compared the pelvic CT images of 17 patients with lymphedema with those of 34 individuals without lymphedema. There were no significant differences in most demographic measures between the two groups, except for the chemotherapy history (Table 1).
Before comparing the patient and normal groups, we compared the patients’ left and right inguinal lymph nodes. The mean number of lymph nodes on the left side was 7.88±1.97 and on the right side was 7.47±1.19. The mean distance of the left-side lymph node from the reference point was 22.65±9.79 mm, and the percentage within the boundary was 77%. The mean distance of the right side from the reference point was 22.29±9.20 mm, and the percentage within the 3-cm boundary was 78% (Table 1). There was no significant difference in the mean number of lymph nodes between the left and right sides (p=0.74). Moreover, there was no significant difference in the mean distance of lymph nodes (p=0.78) or the percentage of lymph nodes within the 3-cm boundary between the two sides (p=0.83) (Table 2).
After determining that there was no significant difference between the left and right sides in patients with lymphedema, we compared the patient and normal groups. The mean number of lymph nodes in the normal group was 6.47±1.19, the mean distance of the lymph node from the reference point was 21.10±9.66 mm, and the percentage of lymph nodes within the 3-cm boundary was 84%. The mean number of lymph nodes in the patient group was 7.68±1.63, the mean distance of the lymph node from the reference point was 22.48±9.51 mm, and the percentage of lymph nodes within the 3-cm boundary was 77% (Table 3). A difference in the mean number of lymph nodes between the normal and patient groups was found (p=0.01). However, there was no significant difference in the mean distance of lymph nodes (p=0.07) or the percentage of lymph nodes within the 3-cm boundary between the two groups (p=0.20) (Table 3).
Discussion
Although VGLNT is an effective treatment modality for lymphedema, it has not been widely used because of concerns regarding donor-site iatrogenic lymphedema [10]. Detailed knowledge of the inguinal lymph node anatomy is essential to avoid postoperative complications. Several authors have reported impaired donor-site lymphatic function and iatrogenic lymphedema following VGLNT [10,11]. Demiri et al [12]. aggregated 11 studies and reported three cases (1.6%) of donor-site lymphedema from 189 patients who had autologous lymph node transfer due to breast cancer-related lymphedema.
Bontumasi et al [8]. examined the CT images of asymptomatic patients and reported that the mean number of SILNs was 10.7 (range, 3–18). Zeltzer et al [13]. also examined the CT images of female patients with breast cancer and reported a mean groin lymph node count of 6.5 with a standard deviation of 2.1. These results are similar to those of our study.
To avoid iatrogenic lymphedema and increase the success rate, anatomical studies on SILN have been conducted [13-18]. Tourani et al [19]. conducted a cadaveric study and recommended using the lateral border of the femoral artery as a readily identifiable anatomic landmark to limit the medial extent of the dissection in VGLNT with a groin donor site.
In our study, 80% of the SILNs were distributed in a 3-cm boundary, which correlates with previous studies. Dayan et al. [5] studied magnetic resonance angiographic images in patients with upper-extremity lymphedema. The group reported that approximately 68% of SILNs are concentrated within a 3-cm boundary extending from a point one-third of the distance from a line drawn from the PT to the ASIS and 3 cm perpendicularly below this line [3,5].
Obesity, radiation, postoperative infection, and even genetic factors are considered significant risk factors for developing secondary lymphedema [5,10]. Therefore, we were concerned about the possible lymph node anatomy difference between individuals without lymphedema and patients with lymphedema and compared the anatomy of inguinal lymph nodes between the two groups. Park et al. [7] reported a high risk of cellulitis with lymphangitis in patients with lymphedema. This could explain the greater number of lymph nodes in patients with lymphedema. The higher prevalence of cellulitis has affected not only the extremity with lymphedema but also the patient’s entire lymphatic system, resulting in activated and enlarged lymph nodes. These lymph nodes may have been visualized better on CT images and thus counted more frequently. Bontumasi et al. [8] studied the mean number of groin lymph nodes as well as their size and shape. In a future study, we could also analyze the size and shape of lymph nodes and compare them between the patient and normal groups.
This study has several limitations. First, the sample size was small. The results could be different if more patients were studied. Second, most of the patients had breast cancer surgery at other hospitals, and we could not obtain detailed information about the patients’ preoperative conditions or the type of breast surgery they had undergone.
There was no significant difference in the distribution of lymph nodes between the two groups, as evaluated by distance and percentage factors. There was a considerable difference in the number of lymph nodes between the two groups (p<0.05). We only could be less concerned about SILN insufficiency when progressing to VGLNT. However, since the detailed knowledge of the functional mechanisms of VGLNT is unknown, it is difficult to conclude the difference in the number of lymph nodes could have a clinical impact. In addition, we can use knowledge from previous anatomic studies, regardless of whether the target group is a patient or a normal group [3,5,8]. Detailed anatomical knowledge on SILN is critical for VGLNT to capture vascularized lymph nodes as well as avoid lymph nodes draining the lower extremity which may cause iatrogenic lymphedema. Current study demonstrated that contrast-enhanced pelvic CT can achieve the detailed image of SILN. Also, CT is an easily accessible and cost-effective method that can be conducted on most patients for personalized SILN anatomy. With the detailed and personalized SILN of the patient, the surgeon will be able to capture vascularized lymph nodes as well as avoid lymph nodes draining the lower extremity.
Conclusion
We could ascertain the detailed anatomy of SILN using CT; hence, we recommend the examination during the preoperative preparation for VGLNT. This study revealed a significant difference in the number of LNs, but no significant difference in the distribution of LNs between the normal and patient groups.