



INTRODUCTION
Tenosynovial giant cell tumors (TGCTs) are typically benign neoplasms of the joint, bursa, and tendon sheath [1]. Until the World Health Organization reclassified them in 2013, TGCT were classified according to their site of origin [2]. According to the 2013 World Health Organization reclassification, the term “localized TGCT” encompasses giant cell tumors of tendon sheaths and nodular tenosynovitis, whereas the term “diffuse TGCT” encompasses diffuse-type giant cell tumors and pigmented villonodular synovitis [2].
Based on the morphology, TGCT can be categorized into two types; localized type (usually located in the digits and wrists) and diffuse type (commonly found around large joints) [3]. The localized type is more prevalent and patients with the located nodular type generally have a long history of tumors that frequently occur as peritendinous fibrous masses in the digits and wrists [4]. In contrast, the diffuse-type TGCT is more aggressive and mainly involves the larger joints such as the hips, knees, ankles, and elbows [5]. TGCT is characterized by hypervascular proliferative synovium containing multinucleated giant cells, macrophages, and hemosiderin [6]. The multinucleated cells express features of osteoclasts. Progressive TGCT near or in the joints limits function and may destroy the adjacent bone [6].
The estimated annual incidence of TGCT is 1.8 to 50 cases per million people [7]. Even though histopathology and genetics are similar between the localized type and diffuse type, the biological behaviors of the subtypes are different. TGCT can occur at any age; however, the localized type is most common in people aged between 30 and 50 years, with a female predominance [8]. Diffuse TGCT generally affects younger patients aged between 20 and 29 years, with no difference according to sex [8]. The localized type is usually benign, while, the diffuse type is more invasive, and may occasionally become malignant.
TGCT typically presents as a small restricted tumor of the hand and wrist, and diffuse TGCT of the small joints is rare [9]. We report a rare case of a huge diffuse TGCT of the wrist and its treatment.
CASE REPORT
This case report was approved by the International Review Board of Soonchunhyang University Hospital (No. 2021-01-035). The patient gave written informed consent for publication of this case report and accompanying images.
We report the case of a 47-year-old male patient with a 10-year history of an asymptomatic nodular lesion on the volar aspect of his wrist. The mass gradually enlarged from the size of a peanut to 60×30×18 mm, and there was no reported history of trauma. The mass slightly reduced the degree of volar wrist flexion but was painless. The radial and ulnar arterial pulses were normal on palpation. The patient had no sensory impairment apart from slight tingling in the dermatome of median nerve. On physical examination, the mass was firm, non-tender, and located on the volar aspect of the left wrist. The mass was free from the skin but attached to the flexor tendons.
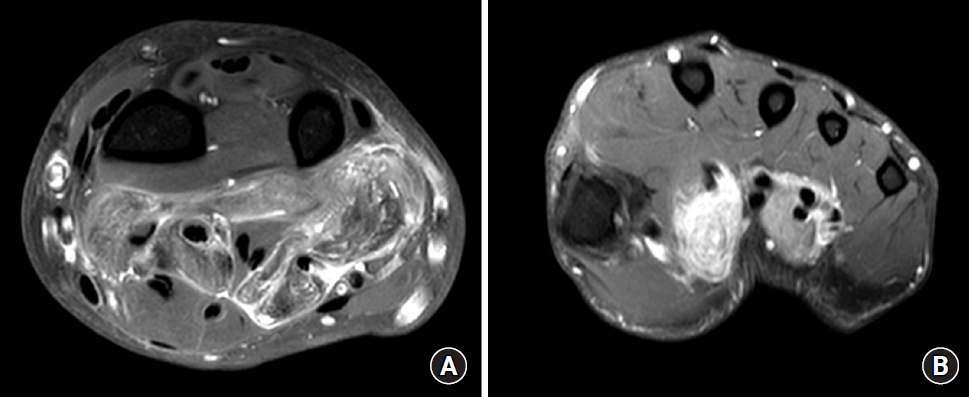
The results of the laboratory studies were as follows; the routine blood tests, antistreptolysin O level, erythrocyte sedimentation rate, high-sensitivity C-reactive protein level, anticyclic peptide containing citrulline level, and other immune indices were normal. The levels of biological markers for the tumor were also normal. A magnetic resonance imaging (MRI) scan showed an extensive multi-lobulated soft tissue mass in the volar aspect of his wrist, arising from the flexor tendons. This mass showed signal intensity similar to the surrounding muscle in T1 and T2-weighted images (WI), and foci of low signal intensity were observed as scattering patterns. Gadolinium T1-WI showed heterogeneous enhancement findings. There was no displacement or penetration of surrounding tissues or direct invasion and no signal change or destruction of the contiguous bony structures (Fig. 1).
We performed surgery under brachial plexus block anesthesia. During the surgery, the tumor was located only on the surface of the flexor tendons. Tumors express colors ranging from dark red-brown to yellow. Tumors are well-circumscribed, with cells growing as solid, often pedunculated nodules attached to the synovial tissue. Although the tumor had a capsule, it had partially infiltrated and damaged the tendons. The tendon sheath was affected (Fig. 2).
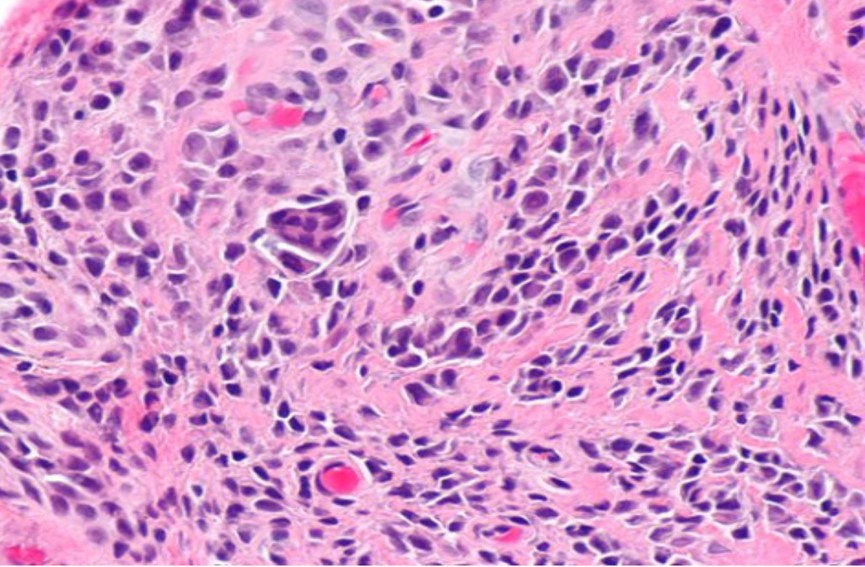
We carefully removed the tumor that surrounding the flexor tendons and performed a carpal tunnel release for the tingling sensation. After excising the tumor, the function of the flexor muscles was assessed, and histological examination of a tissue biopsy revealed that it was a giant cell tumor (Fig. 3). In agreement with the patient, radiotherapy was not performed. The tingling sensation improved, and there was no specific complaint other than a slight joint motion discomfort. He returned to his daily routine two months after the operation. The patient has been followed up for 1 year without recurrence.
DISCUSSION
The cause of TGCT is not yet fully understood. It was first considered to be a tumor, but the possibility of other causes was suggested. Microscopically, TGCT has a range of appearances, variably showing mononuclear cells with a polyhedral and epithelioid appearance, multinucleated giant cells, foam cells, and areas of hemosiderin deposition, arranged in a lobular to diffuse architecture. This appearance led Jaffe et al. and others to believe that an inflammatory etiology was likely. Other possible causes include lipid metabolism, trauma, cancer, and bleeding [10]. More recently, TGCT was found to be a clonal neoplastic process associated with specific genetic changes, frequently due to a specific translocation: t(1;2) colony-stimulation factor (CSF) 1:COL6A3. There is also typically a reactive component with proliferation and recruitment of CSF 1 receptor-expressing cells including macrophages, giant cells, and osteoclasts, in what is known as the “paracrine landscape effect.” [11,12].
Clinical diagnosis is often challenging because of the largely nonspecific symptoms. Radiographs may show bone erosions, although these are often late signs. Computed tomography can provide additional information regarding the extent of bony involvement. However, a definitive diagnosis is only made histologically or by MRI. MRI is currently the diagnostic modality of choice for TGCT, as it can characterize and estimate the extent of soft tissue tumors. Most TGCTs appear isointense relative to the muscles on T1-WI, with variable intensity on T2-WI because of variable hemosiderin, liquid, lipid, fibrous tissue, and hemorrhagic components [13].
Localized TGCT generally occurs in the form of well-delineated lesions that do not penetrate the tendons. However, the diffuse type which is generally aggressive occurs with homogeneous soft tissue masses, and is associated with joint destruction and invasion [14]. The TGCT in our case also aggressively invaded the wrist joint capsule and adjacent flexor tendon. Surgical treatment for locally aggressive diffuse-type TGCT is challenging because pathological tissue can spread widely throughout the joint and adjacent soft tissue and might be technically difficult to remove. In patients with extensive disease, less than radical or only partial resection may be preferred to improve symptoms, with joint preservation in mind. However, higher recurrence rates have been described after macroscopically incomplete resections.
We attempted to remove the mass and perform synovectomy meticulously with preservation of flexor function. Subsequently, the patient complained of a slight joint motion discomfort but had no other specific complaints. This was because the flexor tendons were preserved as much as possible. However, because it was a huge diffuse-type tumor, the possibility of recurrence remains. Also, since the risk of recurrence usually increases over time, the outcome of the current 1-year follow-up does not indicate the final outcome of treatment. Since there is a high risk of recurrence, additional treatments may be considered, and among these, radiotherapy is the most [15,16]. Several studies have evaluated the effectiveness of radiotherapy for TGCT to prevent recurrence. In one meta-analysis of 35 observational studies containing over 600 patients with TGCT of the knee, perioperative radiotherapy was associated with a lower rate of recurrence (odds ratio, 0.31; 95% confidence interval, 0.14–0.70), although the evidence was of low quality [17]. Similarly, in multiple observational cohort studies of patients with diffuse TGCT and in a national pattern of care study, the addition of radiotherapy at a dose of 35–50 Gy was associated with lower local recurrence rates [18]. Despite these results, radiotherapy may cause long-term toxicity and subsequent morbidity, especially in young patients with TGCT, a nonlethal tumor. Examples of such toxicity include joint stiffness due to radiation fibrosis, skin changes, tissue necrosis, and radiation-associated secondary malignancies, including transformation into malignant sarcoma [18,19]. Therefore, we did not utilize this approach.
In patients with suspected recurrence of TGCT, systemic therapies targeting the CSF1–CSF1 receptor axis have been investigated, including nilotinib, imatinib, emactuzumab, and pexidartinib (PLX3397) [9]. Some systemic treatments for patients with TGCT have proven to be active. In particular, pexidartinib (PLX3397) is a novel oral CSF-1R inhibitor that was specifically developed to treat TGCT [9]. This agent similarly showed promising early results in a phase-II trial, with 11 of 14 patients having a 50% reduction in tumor volume [20]. The disadvantages of adjuvant or targeted therapies are acute and long-term side-effects of different degrees, such as fatigue, diarrhea, anemia, hyponatremia, and neutropenia [20].
In an earlier study, Palmerini et al. [21] found that tumor size (<20 mm), macroscopically incomplete resection, male sex, and previous recurrence were prognostic for local failure postoperatively. Several studies calculated recurrence-free survival for patients with diffuse-type TGCT at 3 years, at 5 years, and at 10 years [9]. These results clearly reveal that with longer follow-up, recurrence continues to increase [9]. The patient had no special problems at the 1-year follow-up. However, the patient we treated had a tumor size of more than 60 mm, which was spread diffusely. Furthermore, since the follow-up period of one year is short, additional close follow-up is necessary.
We report a huge TGCT, which grew gradually over 10 years. If the patient’s tumor had not been ignored for 10 years and had been removed earlier, the management may have produced even better results. Although benign, TGCT has a high recurrence rate; hence, early diagnosis and treatment are beneficial.