정상적인 지질 수치를 보이는 환자의 사지에서 발생한 다발성 거대 건황색종
Multiple Huge Tendinous Xanthomas with Normal Lipid Profiles in All Extremities
Article information

Trans Abstract
Xanthomas are grayish-yellow masses composed of lipid-filled foamy histiocytes and are usually accompanied by familial hypercholesterolemia or some other disease associated with dysfunctional lipid metabolism. Here, we report a case of multiple huge tendinous xanthomas with normal lipid profiles involving all extremities. These masses were large enough to cause pain, dysfunction of extremities, and cosmetic compromise and the condition was accompanied by cerebrotendinous xanthomatosis. Due to the presence of many masses in all extremities, a two-stage operation was planned with a time gap of several months. At 1-month follow-up visits after first and second surgeries, although extension of the left middle finger was poor as a result of sacrificing the 3rd extensor digitorum communis tendon, no problems such as wound dehiscence, hematoma formation, or infection at operative sites were noted.
INTRODUCTION
Xanthomas are grayish-yellow masses composed of lipid-filled foamy histiocytes, extracellular cholesterol, giant cells, and inflammatory cells [1], and are usually caused by cholesterol accumulation in familial hypercholesterolemia or some other diseases and may be the mainstay of the clinical diagnoses of these lipid disorders [2]. Xanthomas usually involve skin and subcutaneous tissue, and sometimes involve tendon and bone deeply [3-5]. Tendinous xanthoma usually involves hand extensor tendons, but may also be found on elbow, patella, and Achilles tendons. Several tendinous xanthomas have been reported and are known to be associated with a clinical finding of hyperlipidemia [2,3].
A few case reports have been issued on xanthomas with a normal lipid profile, most concerned plane xanthoma [5] and others tendinous xanthoma of Achilles tendon [6]. Here, we report a rare case of huge multiple tendinous xanthomas in all extremities with a normal lipid profile that were large enough to cause pain, motor disturbance, and poor cosmesis.
Written informed consents was received from the patient for this report.
CASE REPORT
A 68-year-old female patient visited our clinic with a 20-year history of progressively enlarging multiple masses on all extremities (Fig. 1). The patient complained of pain while walking due to multiple huge masses in both feet and motor dysfunction of left middle finger due to huge mass arising from the 3rd extensor digitorum communis (EDC) tendon. She had no systemic symptoms.

The large, firm nontender masses with ulceration were on tendons of left hand, right elbow, both ankles and feet.
Magnetic resonance imaging (MRI) of the left hand showed masses with central necrosis infiltrating the tendon of flexor carpi ulnaris (FCU), flexor pollicis longus (FPL), and the 2nd~ to 4th EDC without definitive involvement of ulnar nerve or artery (Fig. 2). On her right foot, multiple large masses with central necrosis were scanned on the Achilles, peroneus, extensor hallucis longus (EHL), tibialis posterior, and tibialis anterior tendons, and on the left foot, Achilles, flexor hallucis longus (FHL), and EHL tendons were infiltrated by masses. Incisional biopsy of some masses on the left hand and foot revealed they were composed of lipid, foam cells, histiocytes, and lymphocytes (Fig. 3).

In T1-weighted image, xanthoma infiltrated into the tendon of flexor carpi ulnaris was seen in left wrist. There was no definitive involvement of ulnar nerve and artery (arrowhead). The 2nd to 4th extensor tendons were involved by the xanthoma on the left dorsum of hand (arrow).

Histopathology finding showing lipid accumulation (arrow), foam cell (arrowhead), histiocytes, and lymphocytes (H&E, ×400).
Serum cholesterol and triglyceride levels were in normal ranges. Several additional tests were performed to determine the underlying cause. Laboratory testing revealed a serum cholestanol level of 10.11 μg/mL, which confirmed a diagnosis of cerebrotendinous xanthomatosis (CTX) (Table 1). After CTX had been diagnosed, brain MRI was performed but there was no evidence of lipid accumulation in brain parenchyma.

Due to the presence of many disfiguring masses in all extremities, a two-stage operation was planned with a time gap of several months. The upper extremities were operated on first, and lower extremities were addressed during second surgery. Subtotal excision for the masses was done to preserve most tendons and normal function (Fig. 4). However, masses arising from 3rd EDC of the left hand and EHL of both feet (Fig. 5) were completely excised and tendons were sacrificed due to severe infiltration. Biopsy after surgery resulted in diagnoses of tuberous xanthoma for all masses.
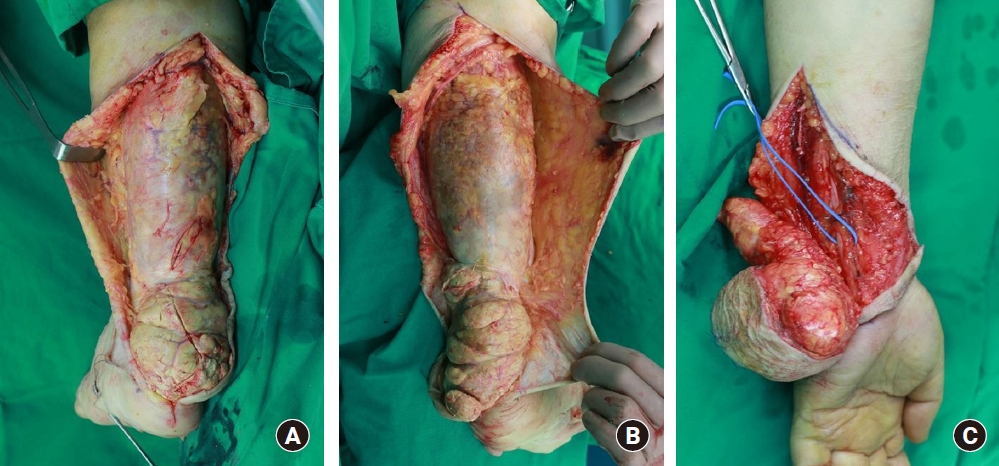
During subtotal excision for mass on the left wrist, ulnar nerve and artery was not involved and preserved (A). (B, C) For the large masses were on both Achilles tendon, subtotal excision was done preserving Achilles tendon.

The masses involved in 3rd extensor digitorum communis tendon (A) and both tendons of extensor hallucis longus (B) was completely excised and then tendons were sacrificed due to severe infiltration into the tendons.
No problems such as wound dehiscence, hematoma formation, or infection at operative sites were noted at 1-month follow-up visits after first and second surgeries, although extension of the left middle finger was poor as a result of sacrificing the 3rd EDC tendon (Fig. 6).

Extension of the left middle finger was poor as a result of sacrificing the 3rd extensor digitorum communis tendon after surgery.
The written informed consent to publish these case details was obtained from the patient.
DISCUSSION
Xanthomas are composed of cholesterol-rich materials and can occur anywhere. They usually accompany familial hypercholesterolemia, though some case reports have described xanthoma in patients with a normal plasma lipid profile [5,6]. Xanthomas usually occur in association with another diseases or syndromes such as CTX, beta sitosterolemia, or overproduction of apolipoprotein B [6-8].
Tendon xanthoma should always be considered in patients with multiple extensor tendon invasions and hypercholesterolemia. However, there is a high possibility of confusing xanthoma with lipoma, nodular tenosynovitis, rheumatoid nodule, or calcinosis cutis [3] when serum lipid profiles are normal, as was observed in our case. Accordingly, proper preoperative imaging, testing, and biopsy are required to determine disease extent and mass characteristics. In our case, xanthoma was confirmed by preoperative biopsy and by extensive invasions of Achilles and multiple extensor tendons of hands as visualized by MRI. Serum cholesterol and cholestanol levels confirmed CTX in our patient.
CTX is an autosomal recessive disorder of bile acid synthesis and was first described in 1937. Deficiency of mitochondrial enzyme sterol 27-hydroxylase leads to excessive cholestanol and cholesterol production and accumulations of these sterols in several tissues. CTX is characterized by intractable diarrhea, neurologic abnormalities, and tendinous xanthomas, especially in Achilles tendons. Sterol analysis or electroimmunoassay is required for the identification of this disease [7].
Several treatment options are available for tendon xanthoma, for example, it could be treated by tendon reconstruction with complete excision, subtotal excision, or amputation. Although Achilles tendon reconstruction or complete tendon removal or amputation have been reported for the treatment of large foot lesions [9], considerations of degree of invasion, functional outcomes, and patient willingness may favor subtotal excision with conservative treatment because total excision for masses with severe invasion on tendons may lead to motor dysfunction sequelae [3]. Of course, subtotal excision may be associated with recurrence, but appropriate medical treatment could prevent or delay this eventuality [10].
In conclusion, xanthoma can occur anywhere and usually accompanies familial hypercholesterolemia. Unlike previous reports, we describe an extremely rare case involving extensive invasion by multiple huge xanthomas in all extremities that caused motion disability and poor cosmesis in a patient with a normal lipid profile that responded satisfactorily to subtotal mass excision.
Notes
The authors have nothing to disclose.